
The Effect of Fluid Availability on Consumption and Perceptual Measures during Aerobic Exercise
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
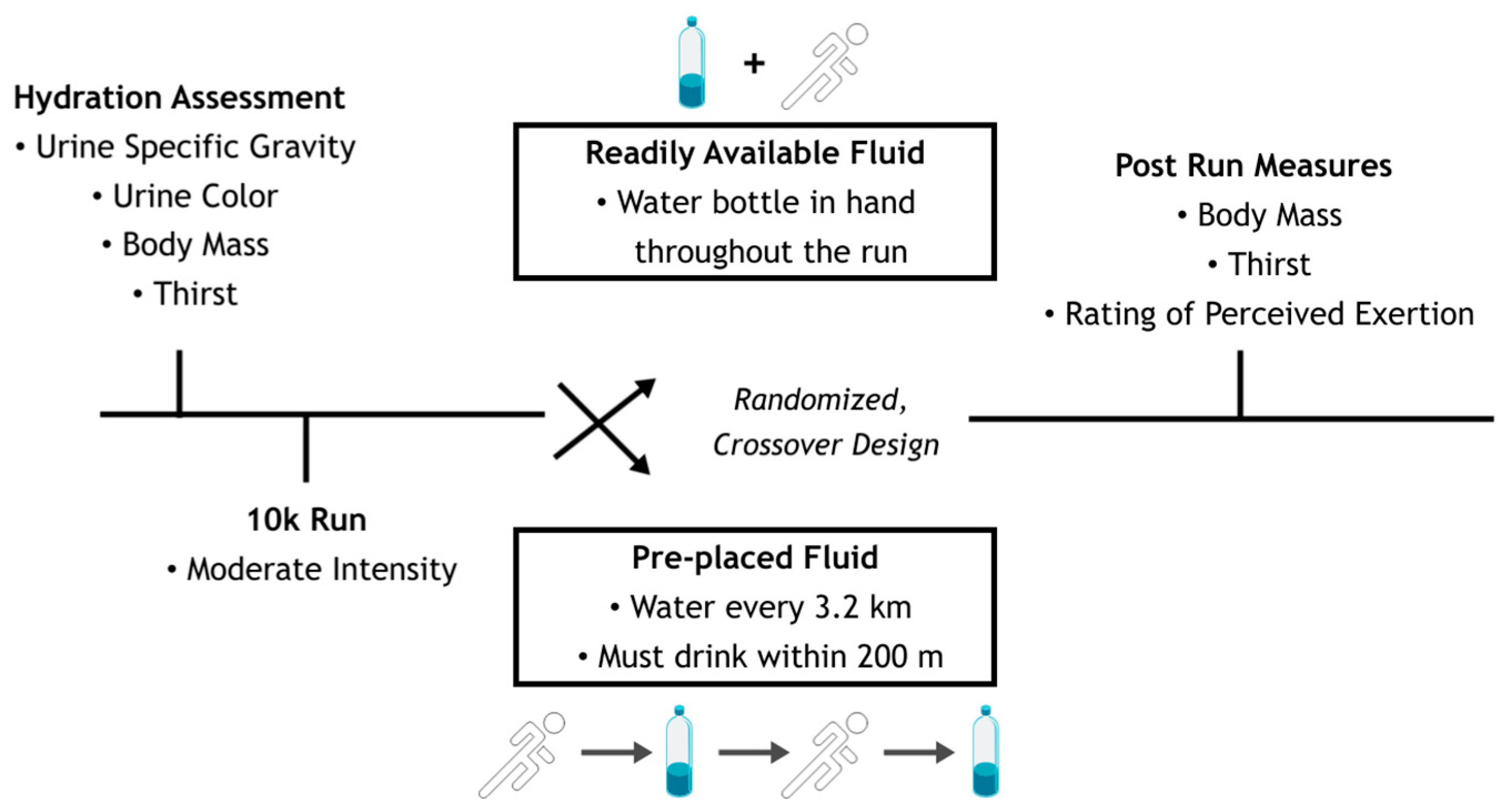
2.2. Study Design
2.3. Study Variables
2.4. Statistical Analysis
3. Results
3.1. Hydration, Heart Rate, and Duration
3.2. Thirst and Gastrointestinal Issues VAS Scale
3.3. RPE and Thirst Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheuvront, S.N.; Kenefick, R.W. Dehydration: Physiology, Assessment, and Performance Effects. Compr. Physiol. 2014, 4, 257–285. [Google Scholar] [CrossRef]
- Ganio, M.S.; Armstrong, L.E.; Casa, D.J.; McDermott, B.P.; Lee, E.C.; Yamamoto, L.M.; Marzano, S.; Lopez, R.M.; Jimenez, L.; Le Bellego, L.; et al. Mild Dehydration Impairs Cognitive Performance and Mood of Men. Br. J. Nutr. 2011, 106, 1535–1543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, J.D.; Sekiguchi, Y.; Suh, H.-G.; Seal, A.D.; Sprong, C.A.; Kirkland, T.W.; Kavouras, S.A. Dehydration Impairs Cycling Performance, Independently of Thirst: A Blinded Study. Med. Sci. Sports Exerc. 2018, 50, 1697–1703. [Google Scholar] [CrossRef] [PubMed]
- Bardis, C.N.; Kavouras, S.A.; Adams, J.D.; Geladas, N.D.; Panagiotakos, D.B.; Sidossis, L.S. Prescribed Drinking Leads to Better Cycling Performance than Ad Libitum Drinking. Med. Sci. Sports Exerc. 2017, 49, 1244–1251. [Google Scholar] [CrossRef]
- Dion, T.; Savoie, F.A.; Asselin, A.; Gariepy, C.; Goulet, E.D.B. Half-Marathon Running Performance Is Not Improved by a Rate of Fluid Intake above That Dictated by Thirst Sensation in Trained Distance Runners. Eur. J. Appl. Physiol. 2013, 113, 3011–3020. [Google Scholar] [CrossRef] [PubMed]
- Kenefick, R.W. Drinking Strategies: Planned Drinking Versus Drinking to Thirst. Sports Med. 2018, 48, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, L.E.; Giersch, G.E.W.; Dunn, L.; Fiol, A.; Muñoz, C.X.; Lee, E.C. Inputs to Thirst and Drinking during Water Restriction and Rehydration. Nutrients 2020, 12, 2554. [Google Scholar] [CrossRef]
- Daries, H.N.; Noakes, T.D.; Dennis, S.C. Effect of Fluid Intake Volume on 2-h Running Performances in a 25 Degrees C Environment. Med. Sci. Sports Exerc. 2000, 32, 1783–1789. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Cotter, J.D.; Goulet, É.D.; Laursen, P.B. VIEW: Is Drinking to Thirst Adequate to Appropriately Maintain Hydration Status During Prolonged Endurance Exercise? Yes. Wilderness Environ. Med. 2016, 27, 192–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passe, D.; Horn, M.; Stofan, J.; Horswill, C.; Murray, R. Voluntary Dehydration in Runners despite Favorable Conditions for Fluid Intake. Int. J. Sport Nutr. Exerc. Metab. 2007, 17, 284–295. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Johnson, E.C.; Kunces, L.J.; Ganio, M.S.; Judelson, D.A.; Kupchak, B.R.; Vingren, J.L.; Munoz, C.X.; Huggins, R.A.; Hydren, J.R.; et al. Drinking to Thirst versus Drinking Ad Libitum during Road Cycling. J. Athl. Train 2014, 49, 624–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buoite Stella, A.; Francescato, M.P.; Sims, S.T.; Morrison, S.A. Fluid Intake Behavior in Athletes during Typical Training Bouts. J. Sports Med. Phys. Fitness 2017, 57, 1504–1512. [Google Scholar] [CrossRef]
- Rivera-Brown, A.M.; Gutiérrez, R.; Gutiérrez, J.C.; Frontera, W.R.; Bar-Or, O. Drink Composition, Voluntary Drinking, and Fluid Balance in Exercising, Trained, Heat-Acclimatized Boys. J. Appl. Physiol. (1985) 1999, 86, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.E.; Kavouras, S.A. Thirst and Drinking Paradigms: Evolution from Single Factor Effects to Brainwide Dynamic Networks. Nutrients 2019, 11, 2864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aragón-Vargas, L.F.; Moncada-Jiménez, J.; Hernández-Elizondo, J.; Barrenechea, A.; Monge-Alvarado, M. Evaluation of Pre-Game Hydration Status, Heat Stress, and Fluid Balance during Professional Soccer Competition in the Heat. Eur. J. Sport Sci. 2009, 9, 269–276. [Google Scholar] [CrossRef] [Green Version]
- Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. American College of Sports Medicine Position Stand. Exercise and Fluid Replacement. Med. Sci. Sports Exerc. 2007, 39, 377–390. [Google Scholar] [CrossRef] [Green Version]
- Engell, D.B.; Maller, O.; Sawka, M.N.; Francesconi, R.N.; Drolet, L.; Young, A.J. Thirst and Fluid Intake Following Graded Hypohydration Levels in Humans. Physiol. Behav. 1987, 40, 229–236. [Google Scholar] [CrossRef]
- Adams, W.M.; Vandermark, L.W.; Belval, L.N.; Casa, D.J. The Utility of Thirst as a Measure of Hydration Status Following Exercise-Induced Dehydration. Nutrients 2019, 11, 2689. [Google Scholar] [CrossRef] [Green Version]
- Batterham, A.M.; Hopkins, W.G. Making Meaningful Inferences about Magnitudes. Int. J. Sports Physiol. Perform. 2006, 1, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Eta-Squared and Partial Eta-Squared in Fixed Factor Anova Designs. Educ. Psychol. Meas. 1973, 33, 107–112. [Google Scholar] [CrossRef]
- Baker, L.B.; Dougherty, K.A.; Chow, M.; Kenney, W.L. Progressive Dehydration Causes a Progressive Decline in Basketball Skill Performance. Med. Sci. Sports Exerc. 2007, 39, 1114–1123. [Google Scholar] [CrossRef] [Green Version]
- Deshayes, T.A.; Jeker, D.; Goulet, E.D.B. Impact of Pre-Exercise Hypohydration on Aerobic Exercise Performance, Peak Oxygen Consumption and Oxygen Consumption at Lactate Threshold: A Systematic Review with Meta-Analysis. Sports Med. 2020, 50, 581–596. [Google Scholar] [CrossRef]
- Arnaoutis, G.; Kavouras, S.A.; Kotsis, Y.P.; Tsekouras, Y.E.; Makrillos, M.; Bardis, C.N. Ad Libitum Fluid Intake Does Not Prevent Dehydration in Suboptimally Hydrated Young Soccer Players during a Training Session of a Summer Camp. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 245–251. [Google Scholar] [CrossRef]
- de Oliveira, E.P.; Burini, R.C.; Jeukendrup, A. Gastrointestinal Complaints During Exercise: Prevalence, Etiology, and Nutritional Recommendations. Sports Med. 2014, 44, 79–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, C.A.; Leib, D.E.; Knight, Z.A. Neural Circuits Underlying Thirst and Fluid Homeostasis. Nat. Rev. Neurosci. 2017, 18, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Leiper, J.B. Fate of Ingested Fluids: Factors Affecting Gastric Emptying and Intestinal Absorption of Beverages in Humans. Nutr. Rev. 2015, 73 (Suppl. S2), 57–72. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean ± Standard Deviation | ||||
|---|---|---|---|---|
| AL | PER | p-Value | Effect Size | |
| Urine Specific Gravity | 1.009 ± 0.008 | 1.009 ± 0.009 | 0.79 | 0.08 |
| Urine Color | 3 ± 1 | 2 ± 1 | 0.22 | 0.39 |
| Body Mass Loss (%) | 1.4 ± 0.6 | 1.3 ± 0.6 | 0.59 | 0.17 |
| Heart Rate (bpm) | 157 ± 11 | 160 ± 11 | 0.22 | 0.40 |
| Exercise Duration (min) | 43.18 ± 0.09 | 42.72 ± 0.12 | 0.41 | 0.26 |
| AL | PER | |||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| How thirsty do you feel right now? | 1.8 ± 1.5 | 4.2 ± 2.5 | 1.7 ± 1.6 | 5.6 ± 2.7 |
| How pleasant would it be to drink some fluid right now? | 4.6 ± 2.0 | 6.8 ± 2.3 | 3.9 ± 2.4 | 7.2 ± 2.8 |
| How dry does your mouth feel right now? | 2.1 ± 1.9 | 4.8 ± 2.1 | 2.3 ± 2.3 | 5.6 ± 2.7 |
| How would you describe the taste in your mouth? | 0.6 ± 0.8 | 2.5 ± 2.3 | 0.9 ± 1.3 | 2.4 ± 2.4 |
| How full does your stomach feel right now? | 4.0 ± 1.7 | 3.8 ± 2.6 | 3.8 ± 2.9 | 3.3 ± 3.1 |
| How sick to your stomach do you feel right now? | 1.6 ± 1.9 | 2.4 ± 2.6 | 1.7 ± 2.3 | 2.8 ± 3.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benjamin, C.L.; Dobbins, L.W.; Sullivan, S.G.; Rogers, R.R.; Williams, T.D.; Marshall, M.R.; Ballmann, C.G. The Effect of Fluid Availability on Consumption and Perceptual Measures during Aerobic Exercise. Int. J. Environ. Res. Public Health 2023, 20, 1310. https://doi.org/10.3390/ijerph20021310
Benjamin CL, Dobbins LW, Sullivan SG, Rogers RR, Williams TD, Marshall MR, Ballmann CG. The Effect of Fluid Availability on Consumption and Perceptual Measures during Aerobic Exercise. International Journal of Environmental Research and Public Health. 2023; 20(2):1310. https://doi.org/10.3390/ijerph20021310
Chicago/Turabian StyleBenjamin, Courteney L., Luke W. Dobbins, Shealyn G. Sullivan, Rebecca R. Rogers, Tyler D. Williams, Mallory R. Marshall, and Christopher G. Ballmann. 2023. "The Effect of Fluid Availability on Consumption and Perceptual Measures during Aerobic Exercise" International Journal of Environmental Research and Public Health 20, no. 2: 1310. https://doi.org/10.3390/ijerph20021310