1. Introduction
In various societal accidents, numerous wounded people die due to massive hemorrhage and ineffective hemostasis [
1,
2,
3]. The development of hemostatic materials with various active components and in different forms to achieve more efficient hemostasis in wound healing has continued to increase during long-term studies [
4,
5,
6,
7]. These commercial hemostatic materials include kaolinite, which is used in combat gauze from Z-Medica Corp. (Wallingford, CT, USA); zeolite, which is used in QuikClot from Z-Medica Corp.; montmorillonite, which is used in WoundStat from TraumaCure Inc. (Bethesda, MD, USA); mesoporous silicon and chitosan, which are used in TraumaStat from Ore-Medix Inc. (Salem, OR, USA); chitosan, which is used in Celox from MedTrade Inc. (Houston, TX, USA) and ChitoGauze Pro from HemCon Inc. (Portland, OR, USA); and cellulose, which is used in Traumastem from Bioster Inc. (Stillwater, MN, USA) [
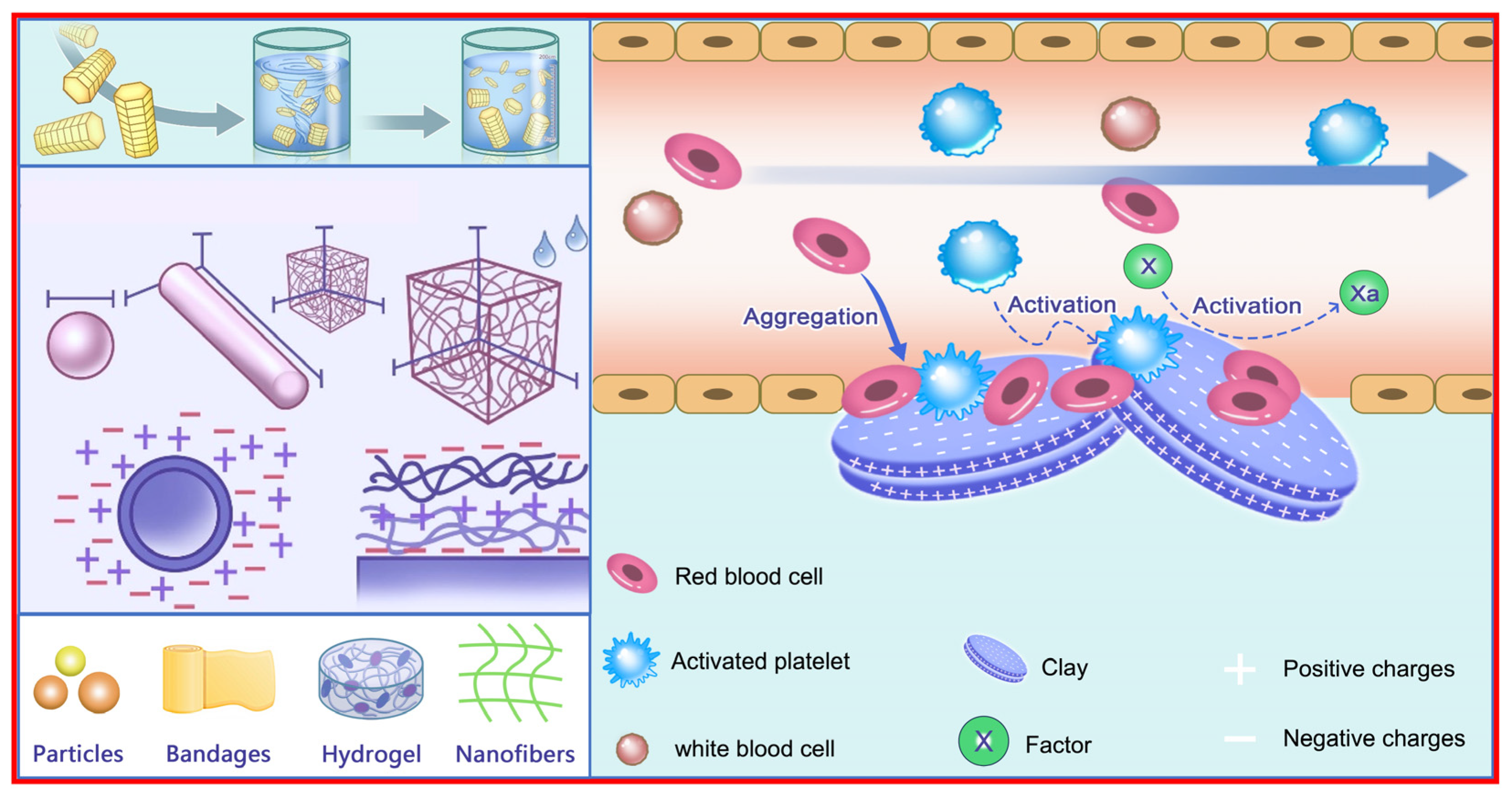
8]. These hemostatic materials act by absorbing water from the blood and concentrating the blood components, activating platelets and blood coagulation cascade reactions, and providing a physical barrier at the hemorrhagic site. In addition, multiple forms, including particles, hydrogels, nanofibers, and sponges, also influence their functions and applications.
Medicinal mineral resources with less market share should be noted, such as cellulose, starch, collagen, chitosan, fibrinogen, etc., because these medicinal mineral resources are distinctive components in traditional Chinese medicine. Their characteristics, including chemical compositions, internal structures, and trace elements, will influence medicinal methods, medicinal efficacies, and remedy-based results. There are more than 80 kinds of medicinal mineral resources, including metals and nonmetals in single-element minerals and compound minerals, which are substances, excipients, or additives in antibacterial, hemostasis, wound healing, and other therapeutic drug applications [
9,
10]. Hemostatic minerals are distinctive and indispensable components in traditional Chinese medicinal mineral resources. They are present in compound minerals, such as stalactite, calcite, limonitum, ochre, kaolinite, montmorillonite, and zeolite, more often than in single-element minerals.
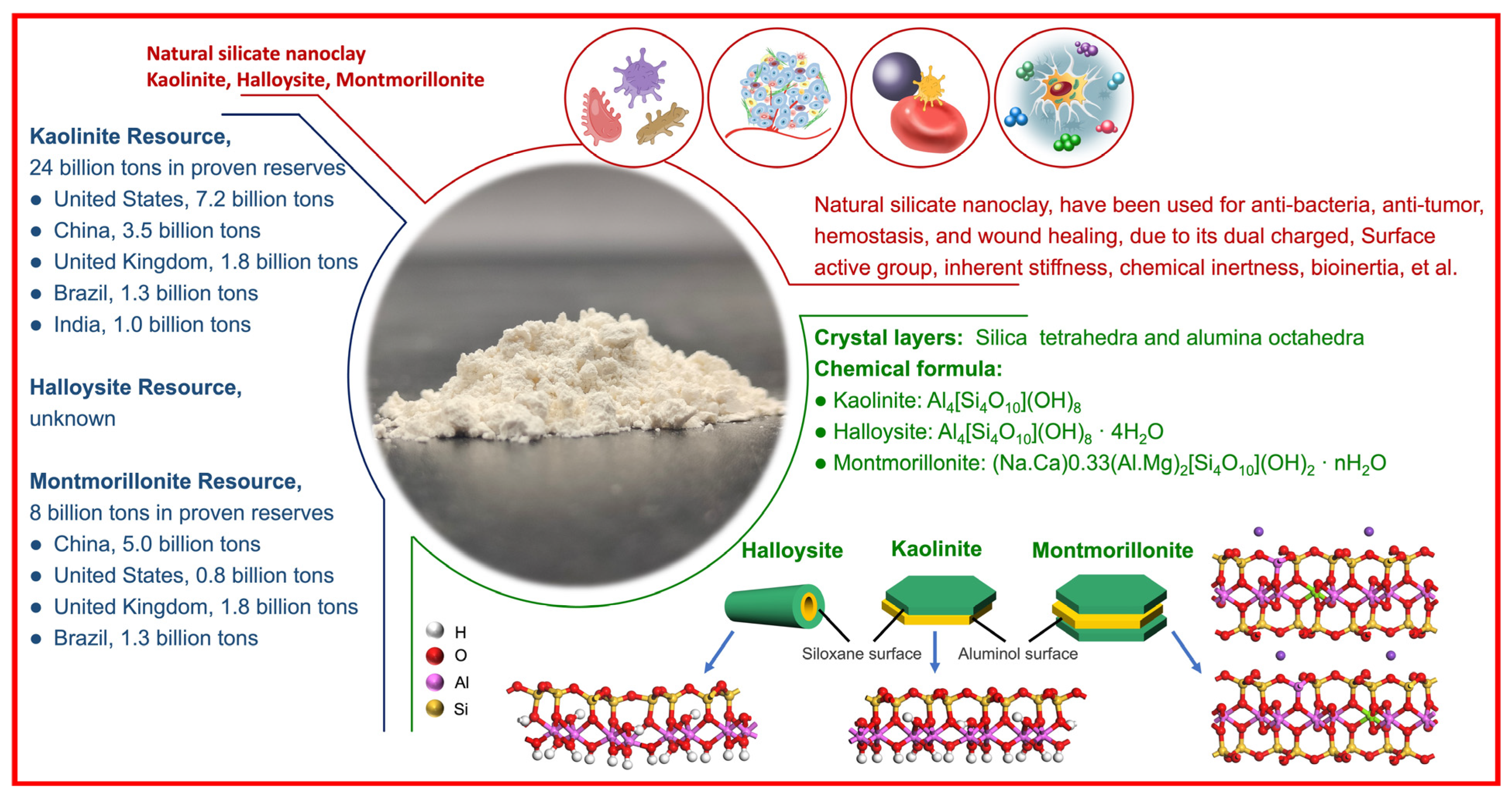
Natural aluminosilicate clay minerals refer to those materials containing Si-O-Al linkages, sometimes accompanied by variable amounts of iron (Fe), magnesium (Mg), titanium (Ti), alkali metals, alkaline earth, and other cations. Natural aluminosilicate clays, such as montmorillonite, kaolinite, halloysite, and diatomite, are used as multinational Food and Drug Administration-approved excipients or additives in various biomedical applications owing to their characteristics, such as natural shape, large specific surface area, high surface-to-volume ratio, dual-charge distribution, active groups, inherent stiffness, chemical inertness, high adsorption and swelling capacities, and biocompatibility [
11,
12,
13,
14,
15]. Kaolinite, with the theoretical chemical formula of Al
2Si
2O
5(OH)
4, consists of one Al-octahedral sheet and one Si-tetrahedral sheet. The active groups include Al-OH groups on the outer surface and Si-OH groups or Al-OH groups on the end face [
16,
17]. Halloysite, with the theoretical chemical formula Al
2Si
2O
5(OH)
4·nH
2O, consists of one Si-tetrahedral sheet-based outer surface and one Al-octahedral sheet-based inner surface. The active groups include Al-OH groups on the inner surface, Si-OH groups on the outer surface, and Al-OH groups or Si-OH groups on the end faces. The dual-charge distribution (negative charges on the outer surface and opposite charges on the inner surface) results from the different groups on the inner surface and outer surface [
18,
19]. Montmorillonite, with the theoretical chemical formula (M
+x+y·nH
2O){(A1
2−xMg
x)[Si
4O
10](OH)
2}, consists of one Al-octahedral sheet and two Si-tetrahedral sheets, where M refers to an exchangeable cation. According to the literature, as of August 2020, there were 222 commercial clay-based commodities with nanotechnologies on the global market, involving 25 countries, 125 companies, and 70 items. The United States ranked first in total, with 66 commodities, 36 companies, and 28 items, and food items were ranked first. China ranked second in total, with 39 commodities, 21 companies, and 16 items, and medicine items were ranked first (
Figure 1) [
20].
In this review, the hemostasis mechanism related to the basic characteristics and chemical composition are studied, numerous wound dressings with different active components and multiple forms are described, and then an outlook for the future is presented.
2. Hemostatic Mechanism
Hemostasis is the first stage in wound healing and immediately starts to reduce blood loss at the wound site in the first minutes. Hemostatic materials are more effective in controlling hemorrhage and even in accelerating wound healing abilities. Therefore, the hemostatic material and its hemostatic biological mechanisms should be summarized in a continuous manner that could be a valuable reference in clinical therapeutics. The hemostatic mechanism for clays is related to their internal structures (one-dimensional or two-dimensional), characteristics (surface roughness, the surface/end charge, and wettable surface), main chemical compositions (silicon, Si; aluminum, Al), trace elements (calcium, Ca; zinc, Zn; copper, Cu; et al.), etc. The nano-bio interactions and hemostatic effects following treatment with clays at the cellular, molecular, and in vivo levels are being revealed.
2.1. Hemostatic Mechanism Related to Material Characteristics
In this section, the hemostatic mechanism related to the surface roughness, the surface/end charge, and the wettable surface are discussed (
Figure 2).
2.1.1. Surface Roughness
Clay surface morphologies, including surface roughness, surface curvature, and surface texture, could affect various protein adsorption properties, including the total adsorption amount, adsorption thickness, competitive adsorption, and conformational changes [
21,
22].
Clays first adsorb plasma proteins in seconds after contact with the blood due to the concentration and diffusion rate in blood. Blood coagulation-related plasma proteins include albumin, γ-globulin, and fibrinogen. Albumin adsorption helps to inhibit blood coagulation on the clay surface. Fibrinogen adsorption and its conformational changes activate blood coagulation factors and platelets, and then thrombi form.
Research has shown that a higher surface roughness results in a larger exposed area in blood and easier clotting; i.e., surface roughness correlates with clotting [
22,
23]. Notably, clay surface modification can enhance surface smoothness, which is beneficial for reducing thrombosis.
2.1.2. Surface Charge
Clay surface charges result from the internal structure, chemical composition, and exchangeable ions of these materials. Clays often have a dual charge distribution and a net negative charge in aqueous suspensions.
Most blood components have a negative charge and can be adsorbed onto clay surfaces with opposite charges through electrostatic attraction, causing coagulation and thrombosis. Notably, a clay surface with a negative charge can activate coagulation factor XII and subsequently cause intrinsic coagulation, even without the adsorption of blood components and cell adhesion [
24,
25].
Research has shown that clay surfaces with different charge distributions and the amount of charge in units influence blood coagulation. Surface modification with the charged groups to obtain a suitable charge distribution range on the clay surface could facilitate blood coagulation.
2.1.3. Wettable Surface and Other Factors
Clay surface groups, including -OH, -COOH, and even -NH
2, could facilitate the formation of a water-wettable region used in protein adsorption [
26]. In addition, clays with higher surface free energy result in larger clay-blood component interactions, which could facilitate protein adsorption and blood coagulation. Notably, clay surfaces with hydrophobic groups could not adsorb those proteins efficiently because of the large interfacial free energies, so blood coagulation activation was needed; that is, the adhesion characteristics between the clay surface and the blood components were much smaller than the cohesion characteristics between the blood components within the blood.
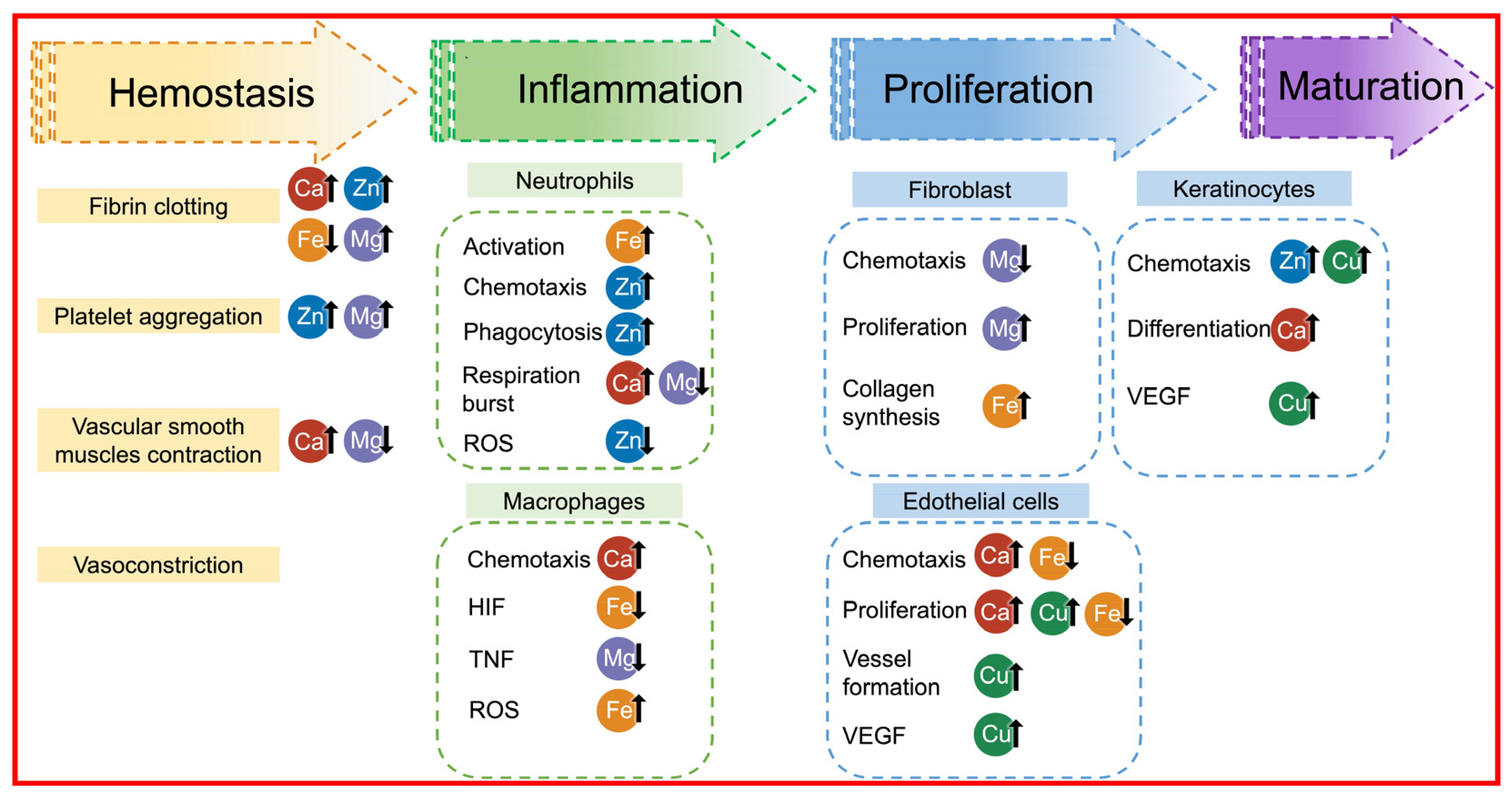
2.2. Hemostatic Mechanism Related to Chemical Components
Aluminosilicate clays mainly consist of SiO
2 and Al
2O
3 and contain certain amounts of Fe
2O
3 and MgO, as well as small amounts of K
2O, Na
2O, and CaO. Skin’s surface environment is weak acidic, and weak acidic environments have been shown to aid wound healing. Metal cations could come out from these metal oxides in weak acidic conditions and even in neutral solutions. Besides, clay surfaces with negative charges tend to attract the opposite cations. In particular, Ca
2+, Zn
2+, Fe
2+, and Mg
2+ can facilitate blood coagulation (
Figure 3) [
27,
28].
2.2.1. Calcium Ions
In intrinsic coagulation pathways, calcium ions can assist in factor IX (FIX) activation and even activate factor X (FX) through combination with activated (FIX). In extrinsic coagulation pathways, calcium ions can accelerate the binding of exposed tissue factor (TF) and factor VII (FVII), which activate FX. In common pathways, calcium ions can facilitate prothrombin transformation into thrombin, assist with phospholipids, and activate FX, which can accelerate fibrinogen conversion into fibrin monomers. In addition, calcium ions can enhance platelet aggregation in platelet-rich plasma and assist in factor XIII (FXIII) activation, which converts soluble fibrin monomers into stable fibrin multimers [
29].
The epidermis is composed of the basal layer, spinous layer, granular layer, transparent layer, and stratum corneum. Keratinocytes are the main constituent cells of the epidermis and are tightly connected by intercellular bridges, forming a barrier. The calcium ion concentration affects keratinocyte proliferation, keratinocyte differentiation, keratinocyte-to-keratinocyte junctions, and keratinocyte barrier function in the epidermis [
30,
31,
32]. The calcium ion concentration inside and outside the keratinocytes from the basal cell layer to the granular layer increases from a low level to a high level, while the calcium ion concentration in the stratum corneum is low. This calcium ion concentration gradient causes the different layers of the epidermis to undergo different degrees of differentiation. Notably, the calcium ion concentration gradient from the inside to the outside of keratinocytes is maintained by the active transport of the cell membrane, endoplasmic reticulum, and inner mitochondrial membrane. The molecular biological mechanism by which calcium ions regulate the division and differentiation of keratinocytes involves increasing the intracellular calcium ion concentration, linking calmodulin with intracellular calcium ions, activating various intracellular enzymes by calmodulin, and regulating the division and differentiation of keratinocytes. Low extracellular calcium concentrations promote keratinocyte proliferation, and high extracellular calcium concentrations promote keratinocyte differentiation and intercellular adhesion.
Various studies have reported the use of calcium-based biomaterials in wound healing [
33]. Calcium-crosslinked alginates have been used for acute and chronic wound healing because calcium ions can assist the clotting cascade [
34]. Moreover, calcium carbonate nanoparticles (topical injection or intravenous injection) and calcium phosphate particles (topical injection or topical dressing) have promoted calcium ion-induced wound healing. During wound healing, calcium-containing bioglass has been shown to promote the proliferation, migration, and protein and growth factor expression of endothelial cells and fibroblasts [
35]. Calcium ions incorporated microporous hydrogel (illustrated in
Figure 4) that could accelerate wound healing through the blood or tissue fluid absorbing on the wound surface due to the hydrogel’s characteristics and activating the coagulation cascade with calcium ions released [
36].
2.2.2. Zinc Ions
Zinc ions are involved in more than 300 enzymes and several transcription factors. During wound healing, zinc ions are involved in epithelial tissue differentiation, metallothionein transport, and storage, reducing UV-induced cell and gene damage and improving the tolerance of skin fibroblasts to oxidative stress [
37].
Zinc ion levels in plasma have a significant effect on hemostasis [
38,
39]. Zinc ions can regulate high-molecular-weight kininogen (HMWK) and factor XII (FXII) to achieve negatively charged surface binding to potentiate the intravascular clotting process. In particular, the combination of HMWK and vascular endothelial cells is important for the activation of FIX and factor XI (FXI) [
40,
41]. In addition, zinc ions can protect calcium ion channels through chelation, ensure the production of calcium-dependent protein kinases during platelet activation, and then facilitate platelet activation [
34]. Clinical research has shown that low zinc intake causes poor platelet aggregation and an increased bleeding tendency in adult males, and this condition can be remedied through zinc supplementation.
Zinc is an essential trace element for maintaining the human immune system and immune cell metabolism. Zinc ions are important for the directed proliferation, apoptosis, and intracellular signaling of immune cells [
42,
43,
44]. Low levels of zinc ions can reduce neutrophil chemotaxis and phagocytosis. Zinc ions are directly involved in protein synthesis, and low zinc concentrations can also affect protein structures and charge states. Zinc ions bind to different amino acid ligands and have different functions, such as maintaining protein structure, redox balance, and cell cycling. For example, zinc ions can affect the ion channel conformation through binding to histidine (His), cysteine (Cys), aspartic acid (Asp), and glutamic acid (Glu) residues. Ion channels are important in various immune cell signaling pathways, especially in T cells and B cells. This explains the indirect effects of zinc ions on intracellular signaling and immune responses [
45].
Zinc ions play an important role in the wound-healing process by supporting tissue growth and repair [
46,
47]. Zinc-dependent matrix metalloproteases can degrade almost all components in the extracellular matrix. These endopeptidases are called matrix metalloproteinases because certain metal ions are required as active sites. These enzymes can originate from several different cells in the wound, such as keratinocytes, fibroblasts, macrophages, endothelial cells, mast cells, and eosinophils. Zinc ion-dependent endopeptidases play important roles in cell proliferation, migration, differentiation, angiogenesis, apoptosis, and host defense [
48]. In addition, zinc is similar to copper and manganese and can enhance autologous debridement and keratinocyte migration during wound healing.
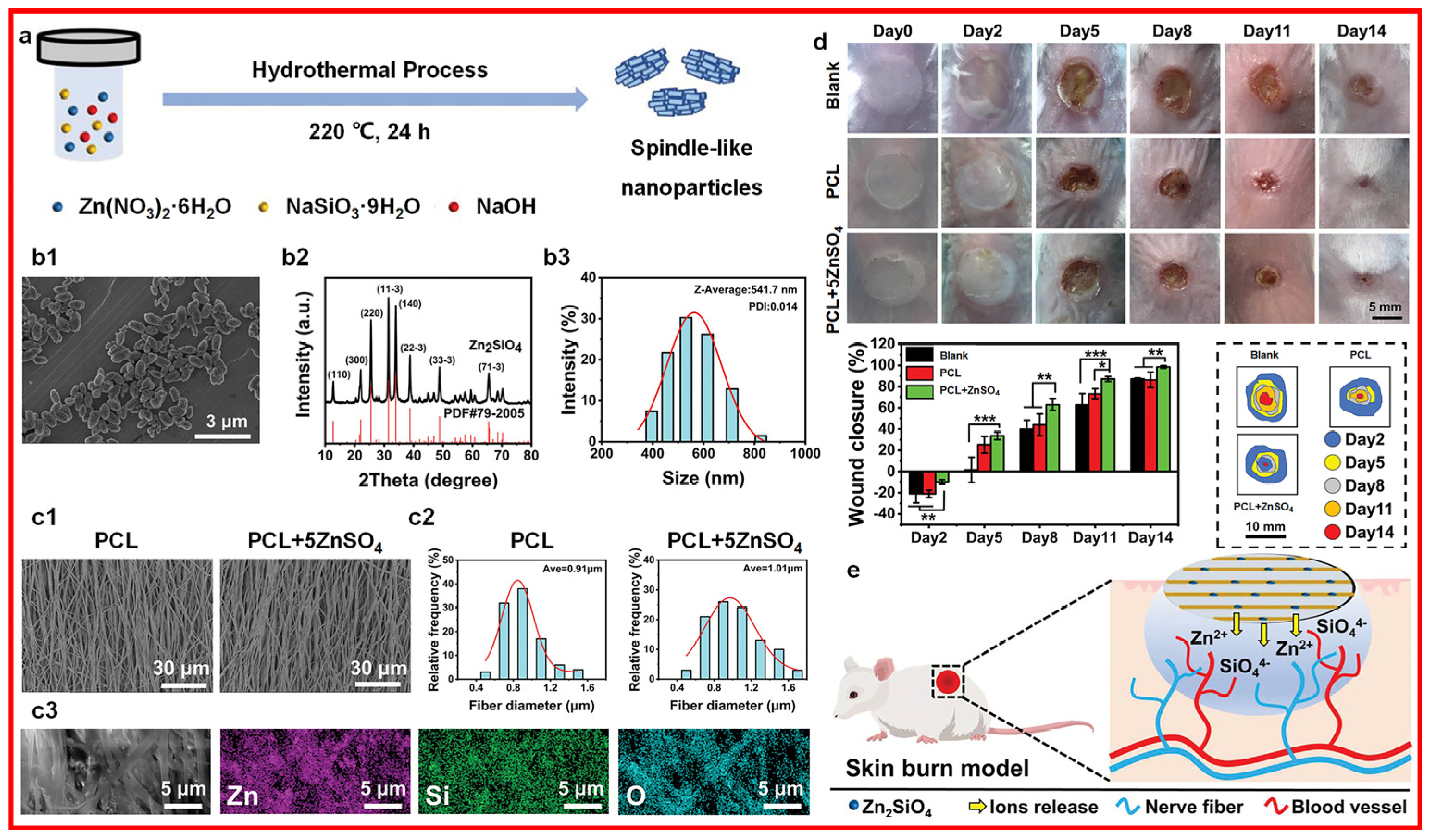
Research has shown that zinc oxide nanoparticles can produce reactive oxygen species (ROS). They can also facilitate cell migration and adhesion and even accelerate the wound-healing process by triggering growth factor-mediated pathways. With the generation of ROS, zinc oxide nanoparticles inhibit the expression levels of superoxide dismutase and glutathione peroxidase genes in human keratinocytes and induce oxidative stress and apoptosis in the cell membrane. Furthermore, the higher zinc oxide nanoparticle concentrations are associated with mitochondrial dysfunction in keratinocytes, releasing lactate dehydrogenase. Zinc ions incorporated scaffold (illustrated in
Figure 5) could accelerate the innervated and vascularized skin burn wound healing through the sustained released zinc ions that could enhance the angiogenic abilities and neurogenic activities in vitro [
49].
2.2.3. Iron Ions
Iron is an indispensable trace element in humans, and its absorption occurs in the duodenum. Most iron exists in red blood cells in the form of hemoglobin, and the free Fe3+ in the plasma can combine with proteins or enzymes to maintain the normal function of the human body. Hepcidin is a peptide hormone that regulates iron homeostasis during iron metabolism, inhibits iron absorption via intestinal mucosal epithelial cells, and regulates the absorption, transport, and utilization of iron in the body.
Thrombin can activate FXIII to generate FXIIIa, convert soluble fibrinogen in plasma into insoluble fibrin monomers, and then the insoluble fibrin monomers interweave into a network to form firm fibrin polymers to achieve rapid hemostasis. Thus, iron ions have a certain influence on fibrin clot formation because iron ions easily combine with protein, Fe
3+ can react with hemoglobin in blood and aggregate into thrombi blocked in blood vessels, and free Fe
3+ modifies fibrinogen molecules for resistant fibrinolysis and stimulates the coagulation cascade reaction, and these phenomena have roles in thrombosis [
50]. Studies have shown that iron oxide nanoparticles can affect thrombin clotting activities [
51]. A lower iron content can cause increased reactive thrombocytosis and then lead to thrombosis. Excess ferrous ions can cause an increase in hydroxyl radicals and then accelerate thrombosis.
Ferrous Fe ions is a prolyl hydroxylase (heme iron(II)-independent dioxygenase) cofactor that could participate in the regulation of hypoxia inducible factor-1α (HIF-1α) hydroxylation during hypoxia. A lower iron ion content results in HIF-1α accumulation due to its stabilization. The increased levels of HIF-1α and vascular endothelial growth factor (VEGF) can be beneficial for angiogenesis and even in wound healing. However, HIF-1α accumulation affects the expression of the proinflammatory cytokine macrophage migration inhibitory factor, which could cause inflammation.
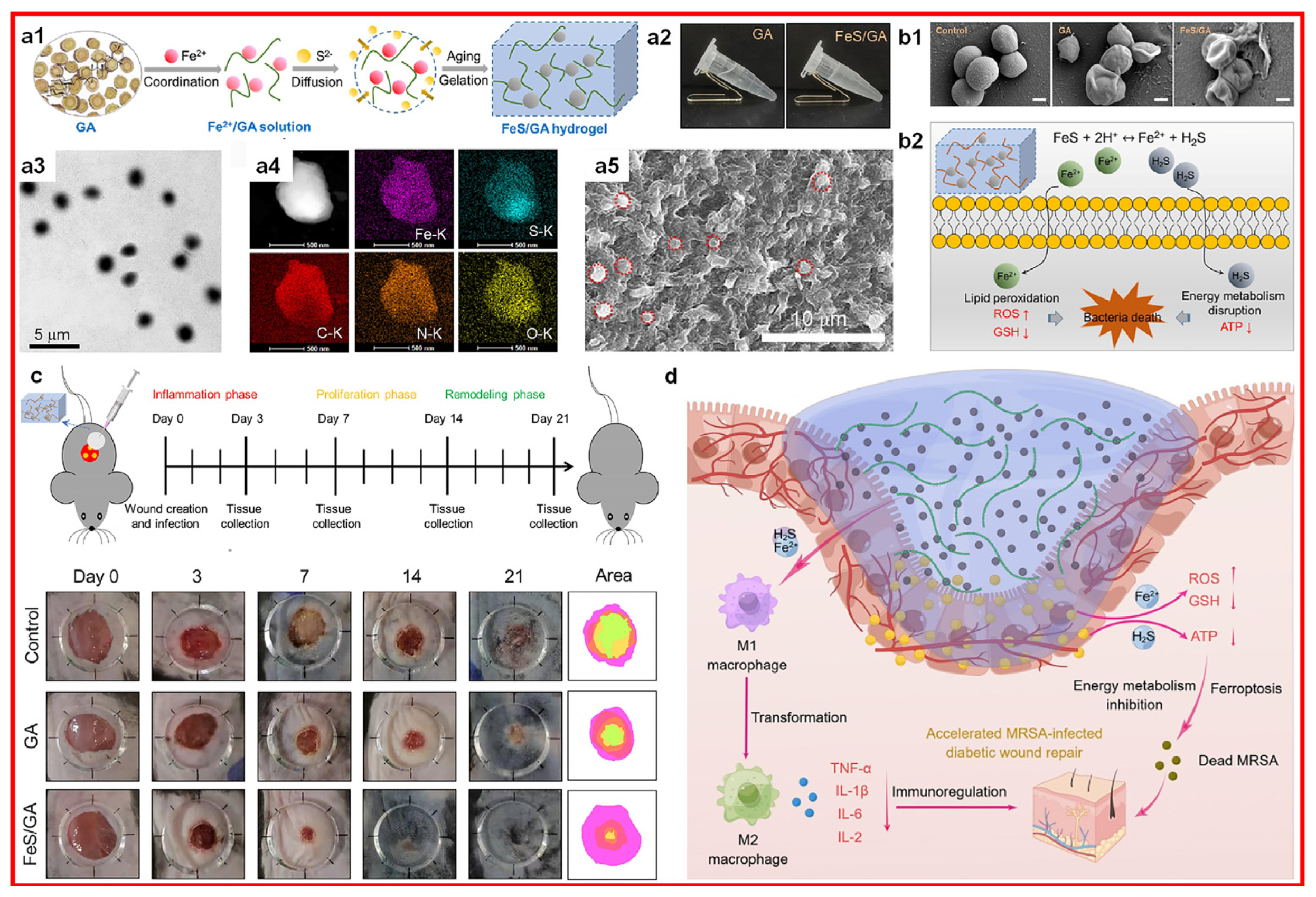
Research has shown that Fe do** and NIR laser irradiation contribute to fibroblast proliferation, neovascularization, and collagen deposition, thus enabling the iron-doped carbon dots-mediated healing of bacteria-infected wounds [
52]. Fe do** endows carbon dots with photo-enhanced peroxidase-like activity, which leads to the generation of heat and ROS to kill gram-positive and gram-negative bacteria. Iron ion incorporated hydrogel (illustrated in
Figure 6) that could accelerate the infected diabetic wound healing through the released ferrous Fe ions that could induce bacterial death [
53].
2.2.4. Copper Ions
Copper is an indispensable trace element in humans, and its absorption occurs in the small intestine and in small amounts in the stomach [
54]. Copper ions have an important role in metabolism because they are important components in metalloenzymes, such as ceruloplasmin, cytochrome C oxidase, copper-zinc superoxide dismutase, tyrosinase, lysyl oxidase, and dopamine-beta-hydroxylase. Therefore, ceruloplasmin could activate ferroxidase and amine chlorinate, which can regulate iron absorption and transport. In addition, copper is a component of coagulation factor V (FV) and metallothionein.
Copper protein plays different roles in biological electron transport and oxygen transport due to the interconversion of Cu
1+ and Cu
2+ [
55,
56]. Cytochrome C oxidase plays a role in oxygen reduction and energy generation. Copper-zinc superoxide dismutase converts superoxide into oxygen molecules and hydrogen peroxide for antioxidant defense. Tyrosinase converts tyrosine into melanin and is involved in collagen synthesis and elastin synthesis in bone and connective tissue. Dopamine beta-hydroxylase has a role in the conversion of dopamine to norepinephrine.
Copper plays an important role in inducing angiogenesis by acting on various angiogenic factors, such as VEGF, angiopoietin (ANG), platelet-derived growth factor (PDGF), fibroblast growth factor 1 (FGF1), fibroblast growth factor 2 (FGF2), and interleukin 1 (IL-1). In addition, copper can affect endothelial cells by binding angiogenin and tripeptide glycyl-L-histidyl-L-lysine (GHK), which then play a role in promoting/modulating dermal wound healing [
57,
58,
59].
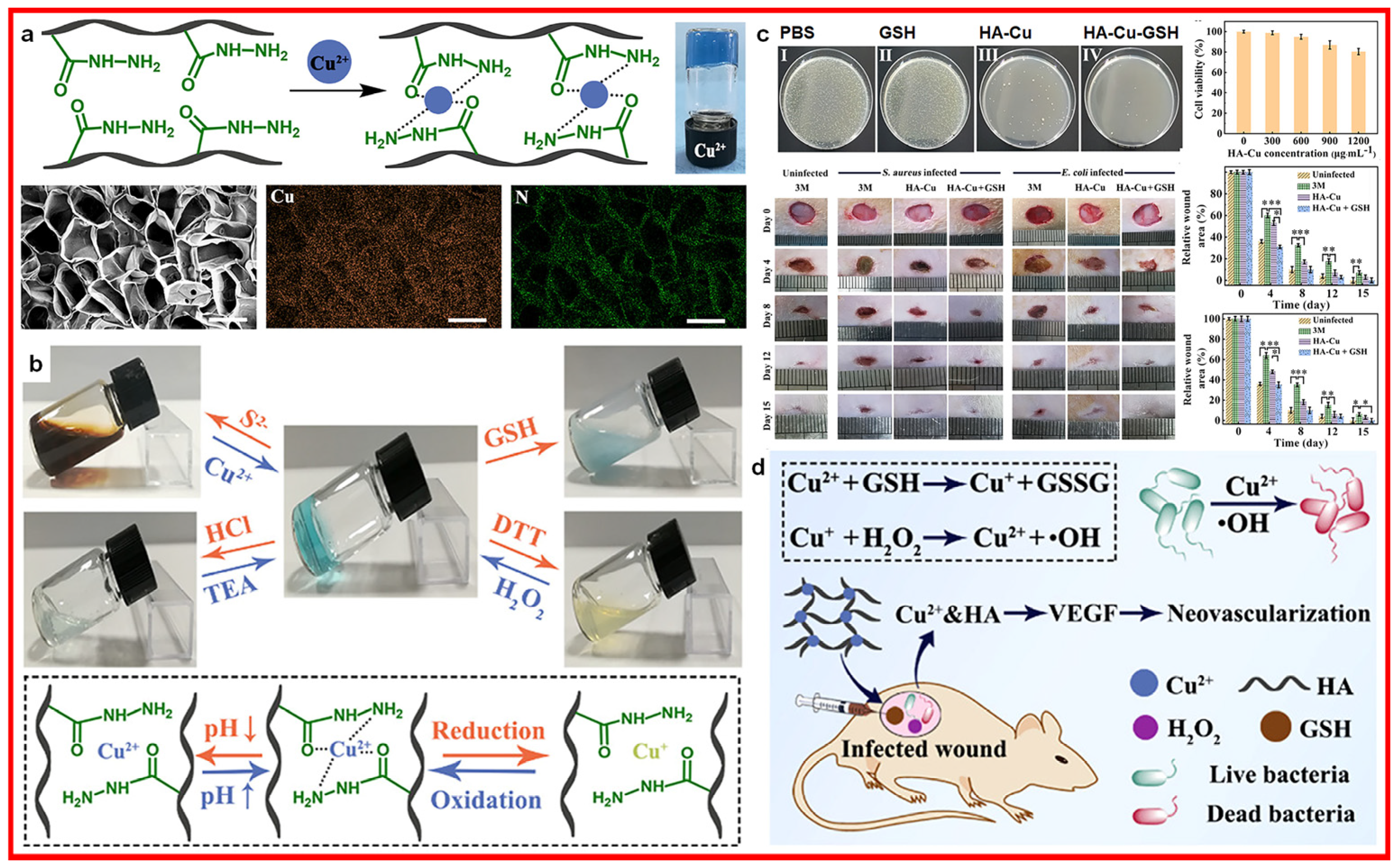
Research has shown that CuS nanodots can be used to treat infected chronic nonhealing wounds [
60,
61]. The released Cu
2+ can promote fibroblast migration and endothelial cell angiogenesis, thus accelerating wound-healing effects. In addition, CuS nanodots with photothermal effects initiate a strong antibacterial effect on drug-resistant pathogens, including methicillin-resistant
Staphylococcus aureus (MRSA) and extended-spectrum beta-lactamase
Escherichia coli, both in vitro and in vivo. Copper ion-incorporated hydrogel (illustrated in
Figure 7) impacts the healing of infected wounds through the released copper ions, which could induce bacterial death [
62].
2.2.5. Magnesium Ions
Magnesium exists in the form of Mg2+ in humans and can serve as a cofactor in multiple enzyme catalysis reactions, participate in energy generation and transportation, coordinate protein synthesis, help transmit nerve signals, and keep muscles loose. Magnesium ions play a protective role in cardiovascular diseases, such as inhibiting calcium channels and potassium channels, inhibiting calcium ion deposition on the blood vessel wall, and creating stones. Approximately 60–80% of magnesium ions in humans are found in mitochondria, bones, myocardium, and cells.
Magnesium ions play an important role in activating coagulation FVII. However, magnesium sulfate mainly shows antithrombotic properties by inhibiting platelet aggregation and thrombus formation. In addition, magnesium ions can modulate vascular smooth muscle contraction by competing with calcium in calcium channels. Fewer magnesium ions can lead to coronary atherosclerosis or thrombosis.
Magnesium ions can promote the proliferation and migration of human umbilical vein endothelial cells and the formation of collagen and angiogenesis in skin wounds. Magnesium ions enhance the migration and adhesion of human skin fibroblasts and human immortalized keratinocytes [
63,
64,
65]. Magnesium ions can promote Zn
2+ into human skin fibroblasts by upregulating the expression levels of the zinc and its transporter 6/10 (ZIP6 and ZIP10) genes, enhancing signal transducer and activator of transcription 3 (STAT3) phosphorylation to induce human skin fibroblasts to differentiate into myofibroblasts, and accelerating the deposition of extracellular matrix, thereby promoting the wound healing of skin tissues [
66].
Magnesium ions play an important role in immune cells and affect immune function. Magnesium ions are involved in immunoglobulin synthesis and complement activation, regulating macrophage phagocytic function and T lymphocyte maturation. In addition, magnesium ions are anti-inflammatory agents that have immune protection effects in eliminating excessive inflammation.
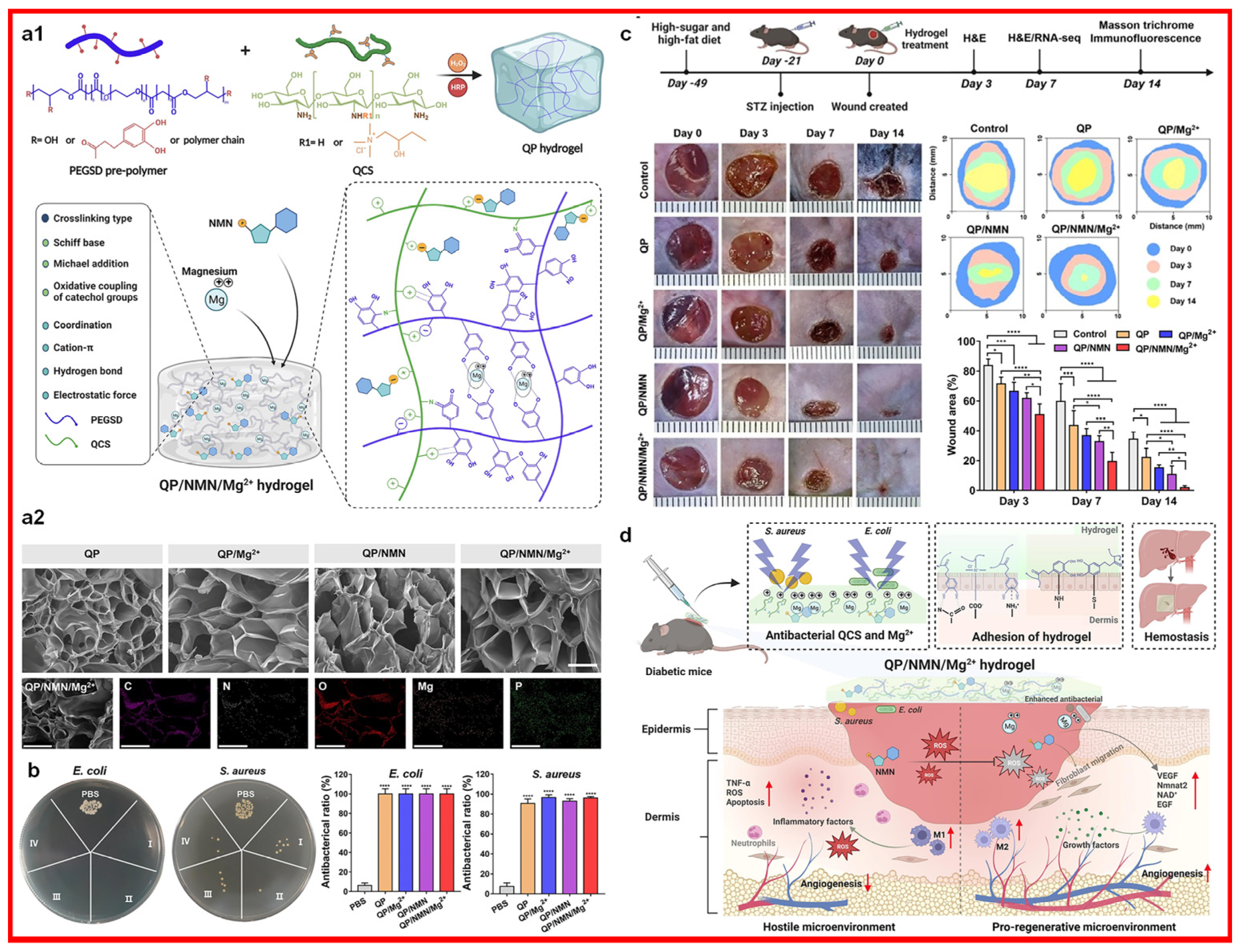
Research has shown that magnesium ions can inhibit the production of the proinflammatory cytokines (tumor necrosis factor-α, TNF-α; interleukin 6, IL-6) in macrophages and the production of ROS and NO in immune cells, thus attenuating the neutrophil respiratory burst [
67]. Magnesium ion-incorporated hydrogels are confirmed to have good proliferative capacities for fibroblasts and good inhibition effects on the NF-κB pathway (a classic transcription factor associated with inflammation and infection) [
68]. Magnesium ion incorporated hydrogel (illustrated in
Figure 8) could accelerate the healing of infected diabetic wounds through the released magnesium ions, which could induce bacterial death and increase the M2 macrophage count [
69].
2.2.6. Other Ions
In addition to the abovementioned ions, other ions, such as aluminum ions, silicon ions, and manganese ions, play less of a role in hemostatic effects. Aluminum ions combine with fibrinogen, accelerate the adhesion and activation levels of platelets, and then promote thrombosis [
70]. Silicon ions can affect the adsorption of extracellular matrix components, such as collagen I, fibronectin, and vitronectin. Manganese ions can shrink local tissue [
71].
4. Conclusions and Outlook
Clays are used in biomedical fields, such as antibacterial, hemostasis, and wound healing, and have received international attention. Basic exploration and technical research related to the fine processing and functional manufacturing of clays have basically eliminated the need for empirical identification techniques, such as sources, characteristics, physical clay resources, and chemical clay resources, and they have greatly reduced the dependence of clay resources on types, reserves, and grades. The following issues include the technologies regarding value- and effect-added medicinal resources, the evaluation methods regarding bio-safe medicinal materials, the wound healing mechanism at different levels, and wound dressings with different active components and multiple forms, which is something that needs to be studied in the future.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}











