
Differences in Dynamics of Lung Computed Tomography Patterns between Survivors and Deceased Adult Patients with COVID-19



Abstract
:1. Introduction
Purpose of the Article
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
3. Results
3.1. Clinical Information
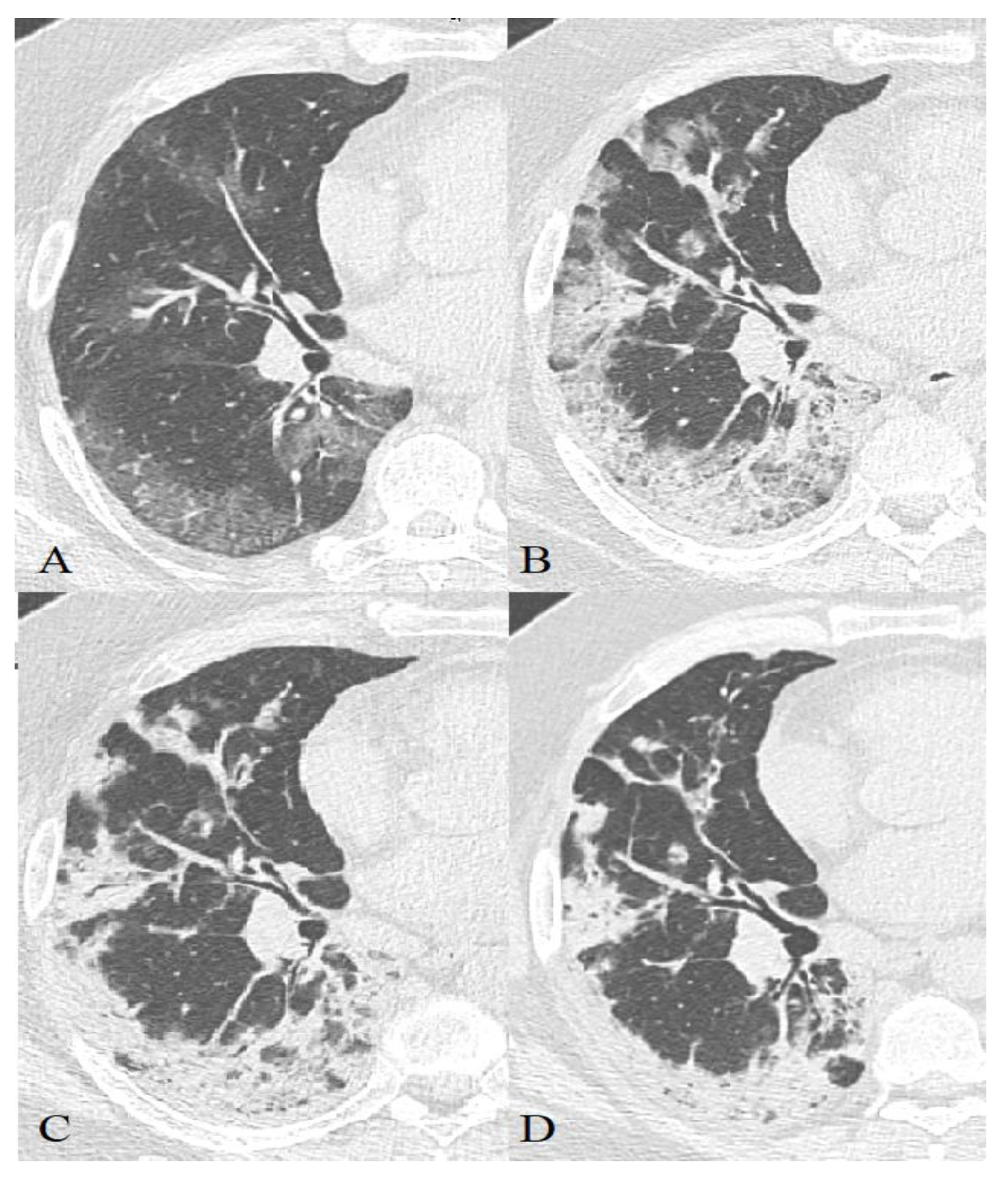
3.2. CT Manifestations of Coronavirus Infection
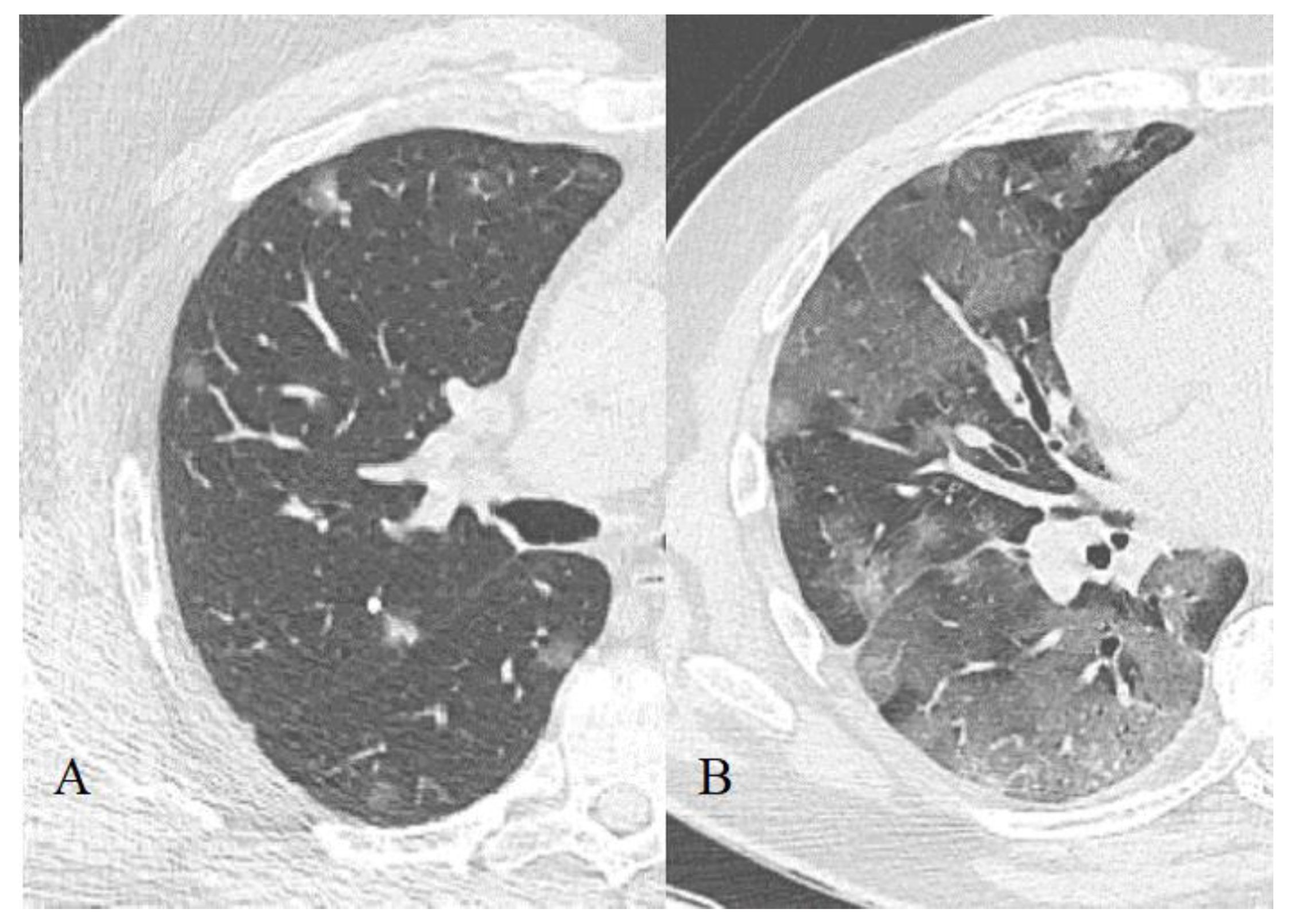
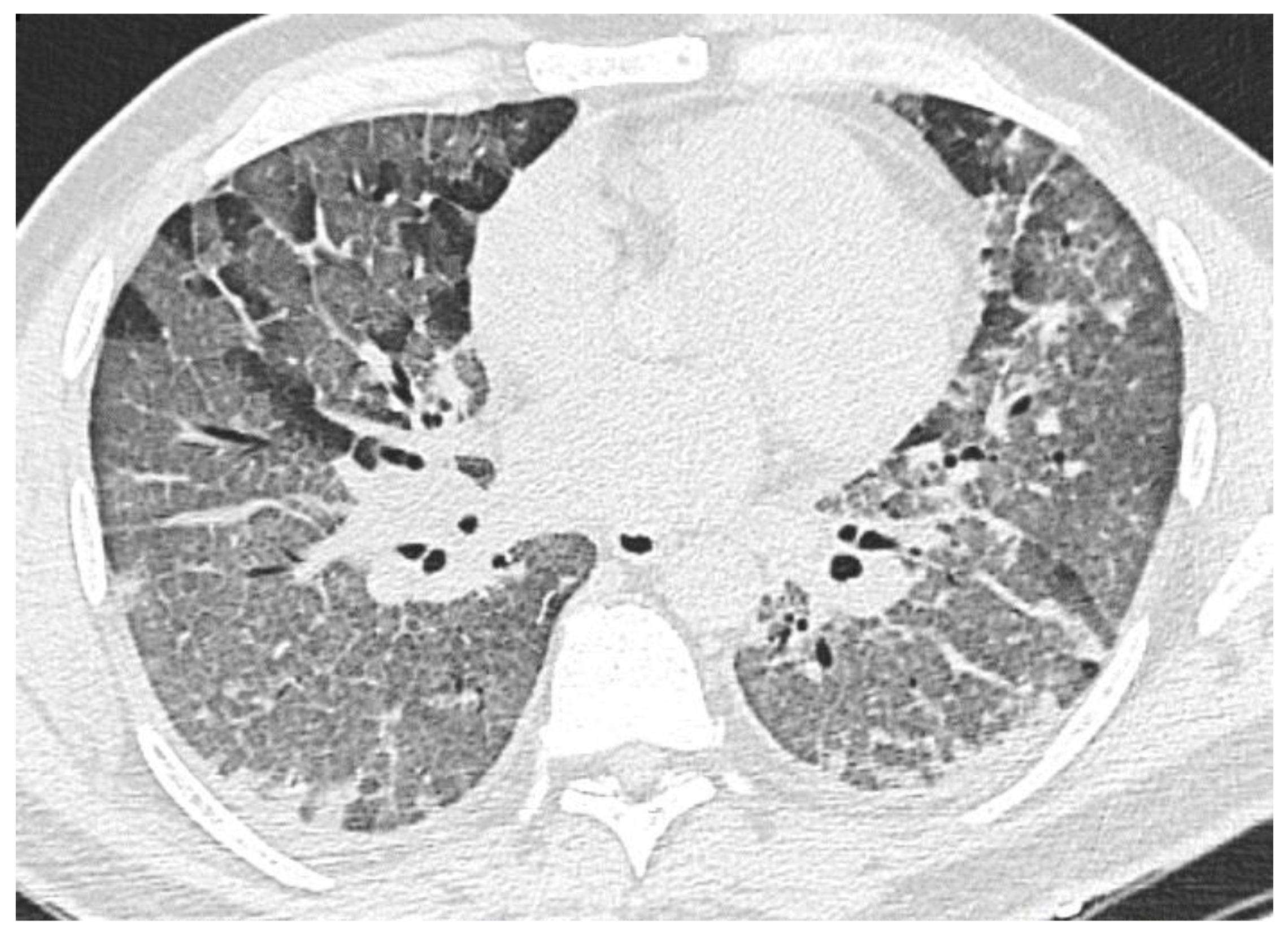
3.2.1. Ground-Glass Opacity
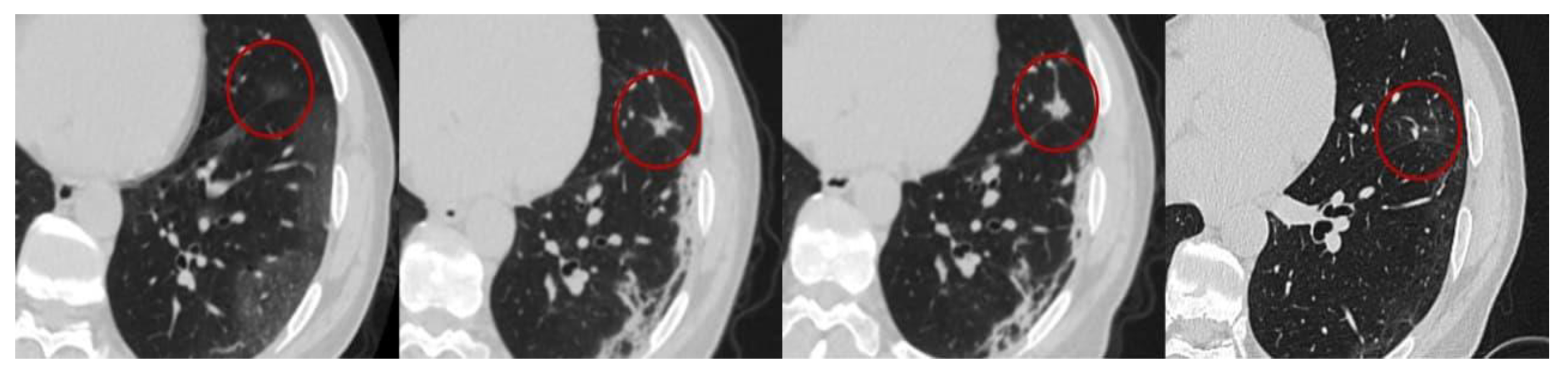
3.2.2. Consolidation
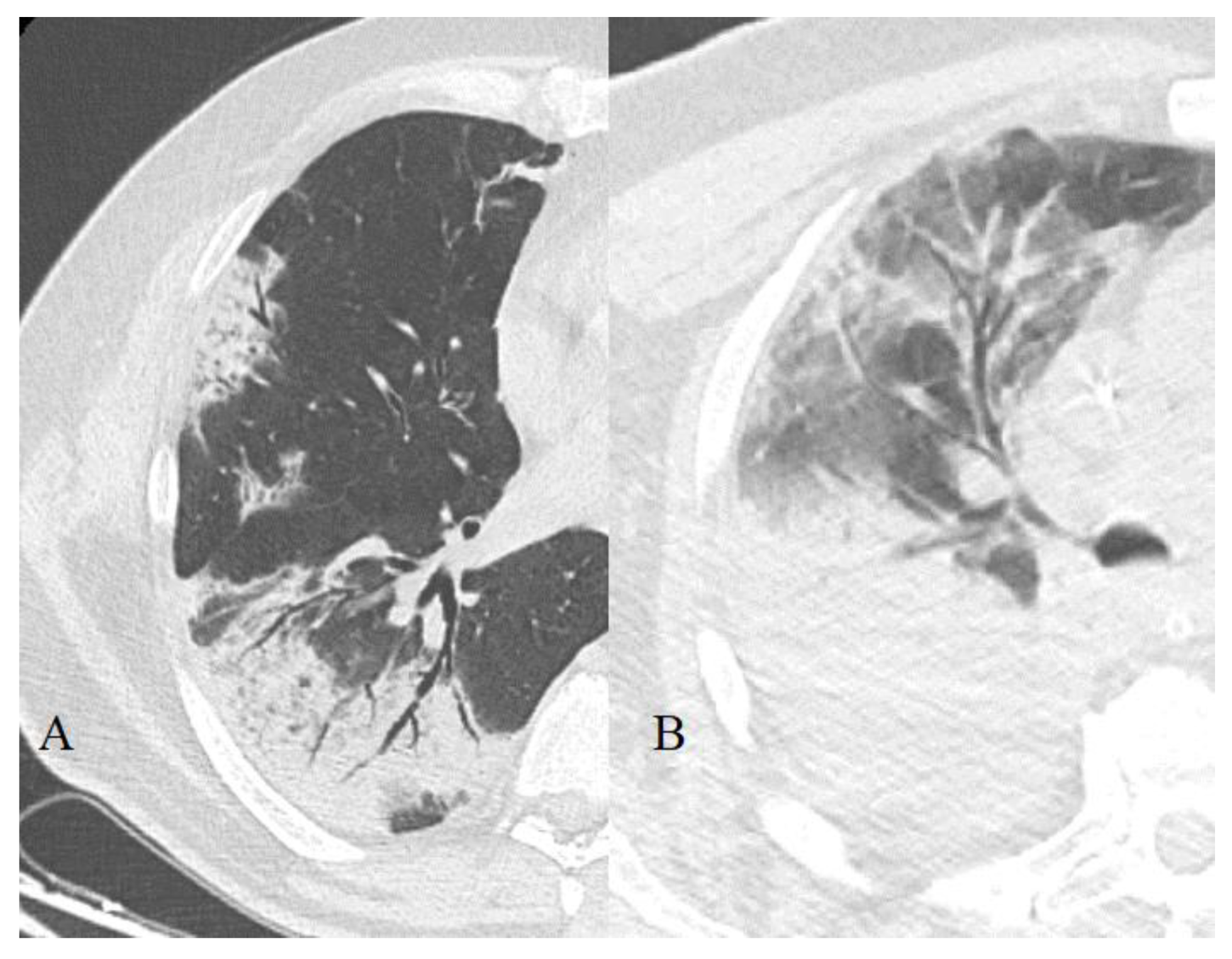
3.2.3. “Crazy Paving” Pattern
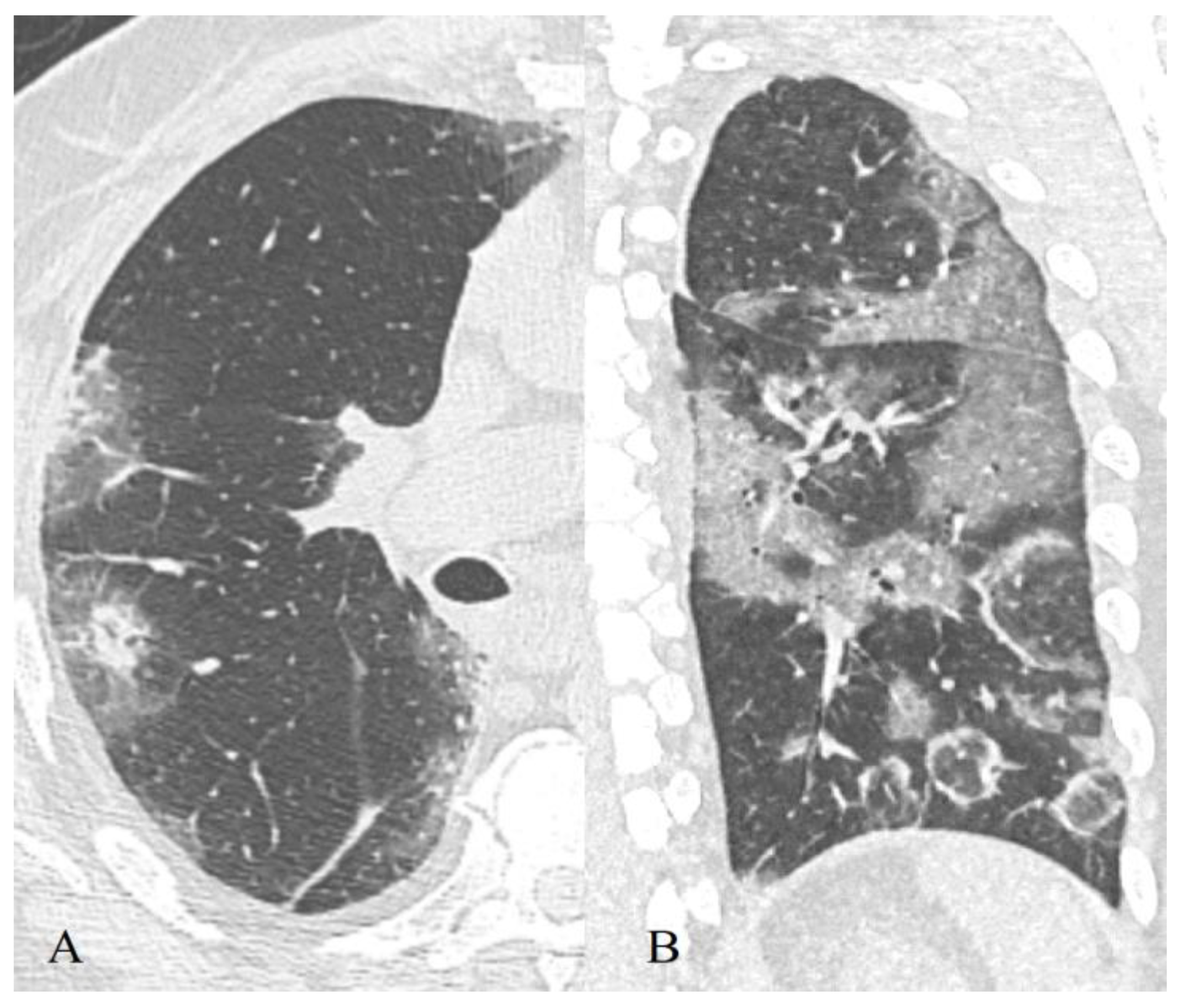
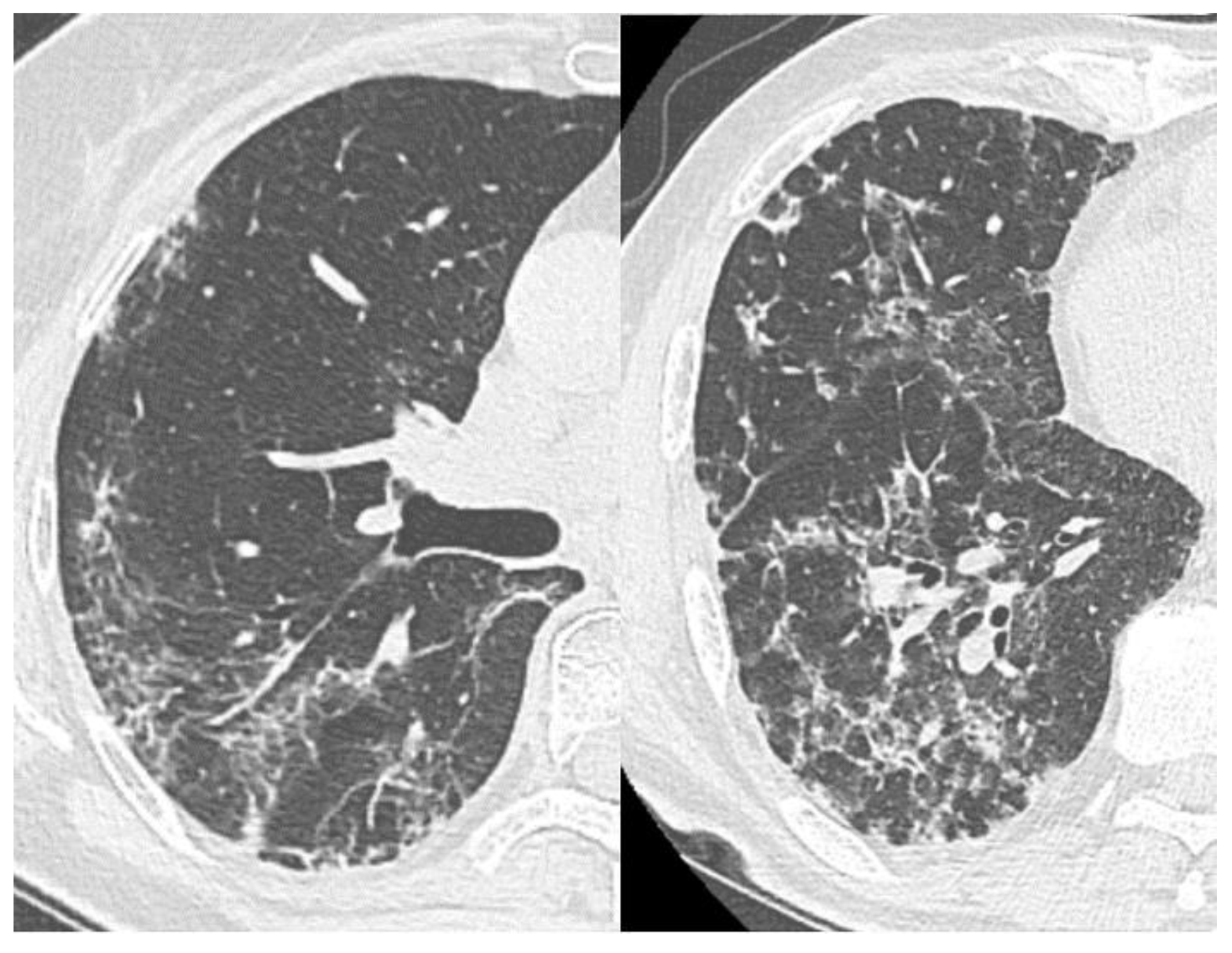
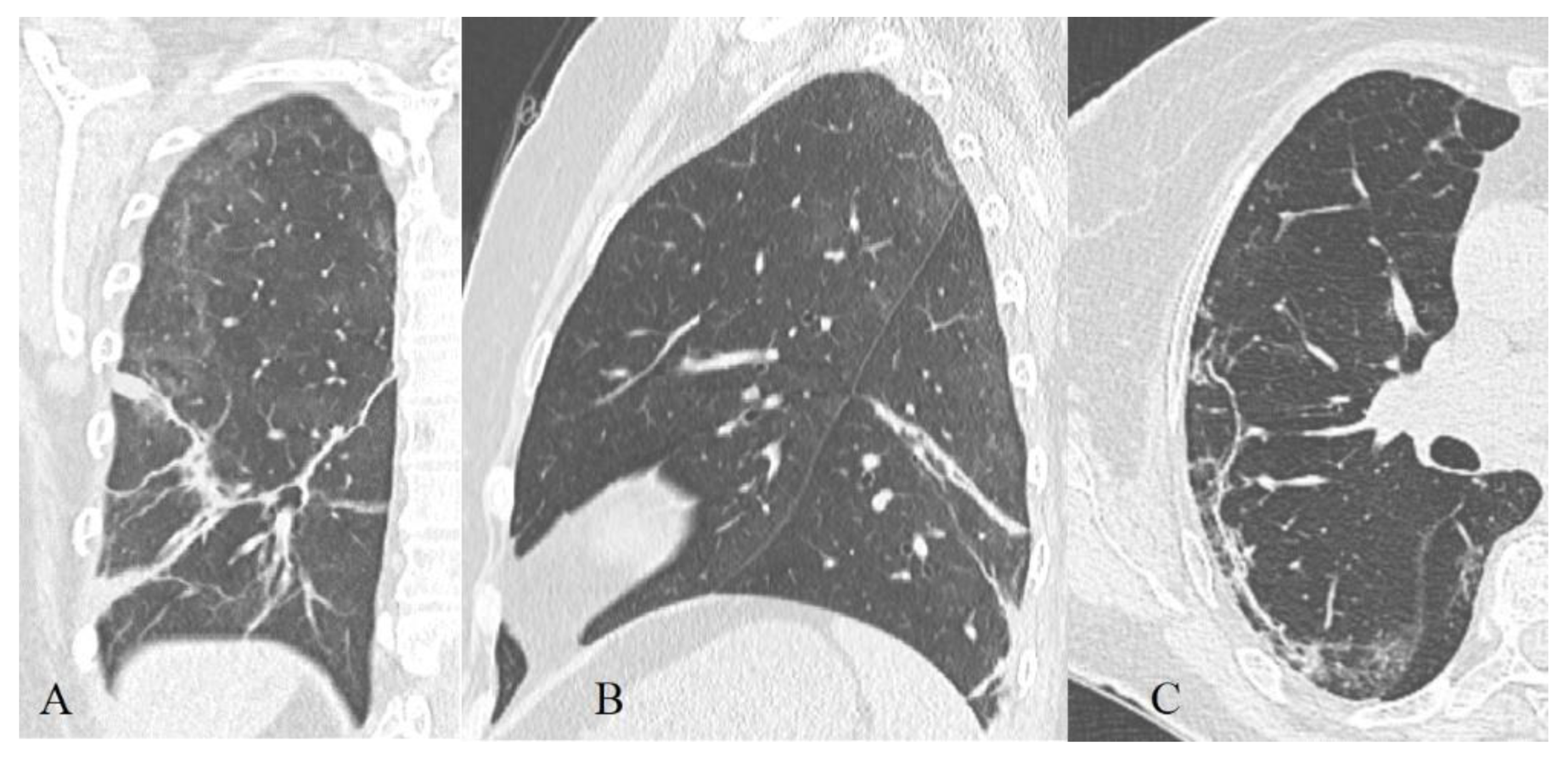
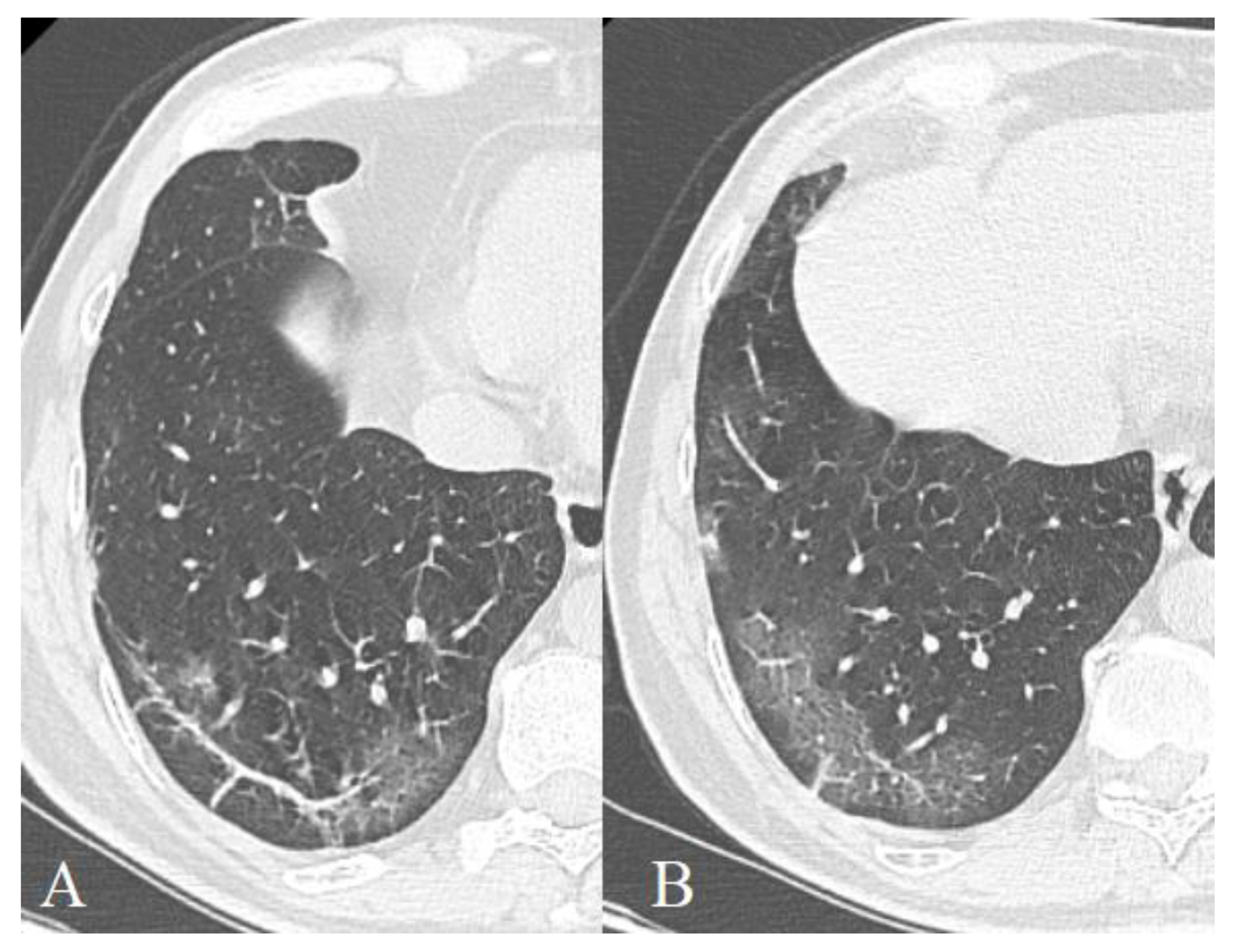
3.2.4. Reticular Interstitial Pattern, Pleuroparenchymal Bands
3.2.5. Localization, Shape, and Volume of the Lesion
3.2.6. Hydrothorax, Hydropericardium, Lymphadenopathy
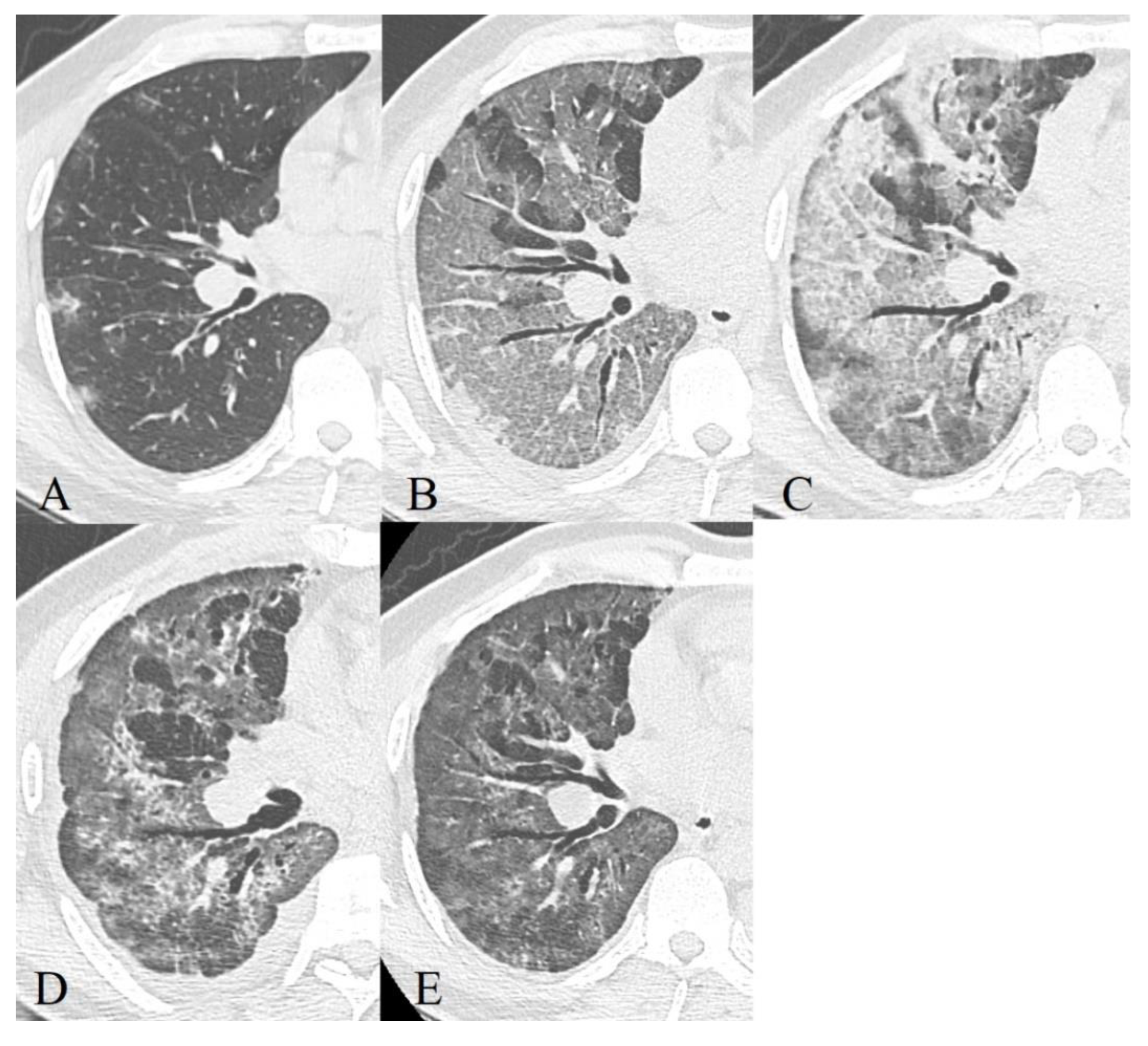
3.3. Dynamics of CT Changes over Time
- Early or initial (0–4 days): normal CT scan or the presence of areas of the GGO type;
- Progressive (5–8 days): an increase in the volume of the GGO type lesions (the frequency of isolated registration is ~40%) and the appearance of CP zones; a combination of GGO and consolidations (in ~43%), GGO and RC (in ~58%); the presence of only consolidations (in ~12%) [43];
- Peak (9–13 days): a significant decrease in the frequency of isolated GGO type changes with a predominance of a combination of GGO and RC (the combination of GGO and consolidations occurred in 30% of cases and already showed a downward trend, in 13% of cases there was a development of pleural effusion, compared to 2.3% during the previous phase) [43];
- Resolution (>14 days): an increase in the volume of the air pulmonary parenchyma with the appearance and predominant contribution of RC, parenchymal bands, and subpleural lines, a reversible halo (signs of organizing pneumonia). At the same time, there is a decrease in the contribution of the combination of GGO and consolidations to the overall CT picture (~9%), with the beginning of a downward trend in the contribution of the combination of GGO and RC (~66%). The contribution of the isolated GGO pattern remained unchanged in comparison with the previous phase (~22%) [43] since consolidation was probably resolved into GGO.
- Early or initial (0–4 days): GGO type changes dominated in both cohorts, but almost 67% of deceased CT studies had CP pattern in this phase of disease, almost half of studies demonstrated mixed GGO-consolidation changes;
- Progressive (5–8 days): an increase in the volume of the GGO, appearance and increase CP (56% of recovered patient’s studies, 73%—deceased), consolidations (57% of recovered patient’s studies, 87%—deceased) type lesions in both cohorts, RC presented in half of the studies;
- Peak (9–13 days): predominance of a combination of GGO (87%), consolidations (67%), and RC (54%) in recovered patients and the combination of CP (87%), consolidations (77%) and RC (65%)—in deceased. RC demonstrated ascending trend in both cohorts, consolidations—in recovered patients, CP—in deceased, the contribution of GGO decreased in both;
- Resolution (>14 days): predominant contribution of consolidations and RC in both cohorts, at the same time there is a decrease in the contribution of GGO, but CP contribution decreased more slowly in deceased than in recovered patients.
3.3.1. Severity of Lung Damage
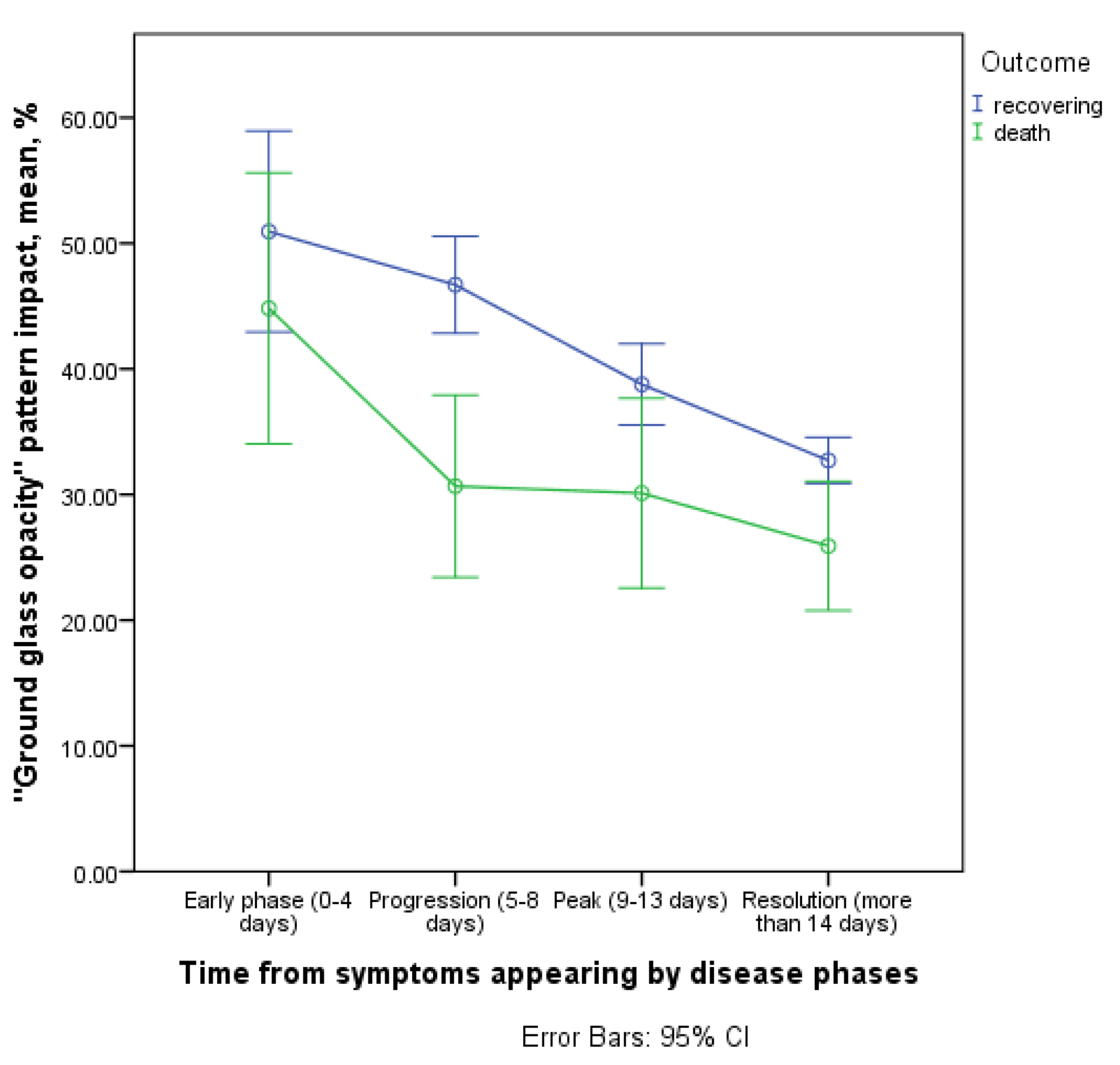
3.3.2. Contribution of the ‘GGO’ Pattern to CT Picture in the Affected Areas
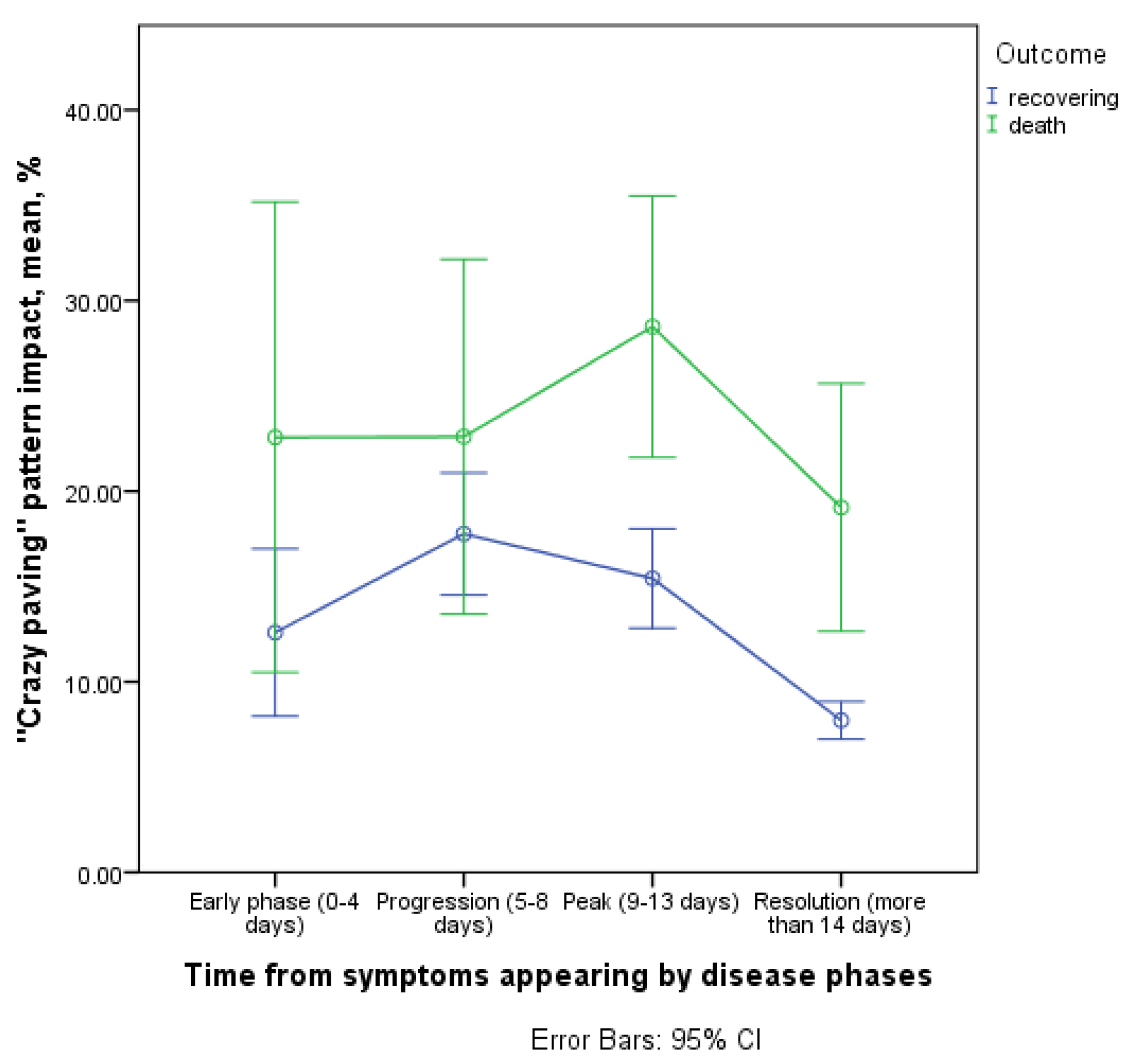
3.3.3. Contribution of the ‘Crazy Paving’ Pattern to CT Picture in the Affected Areas
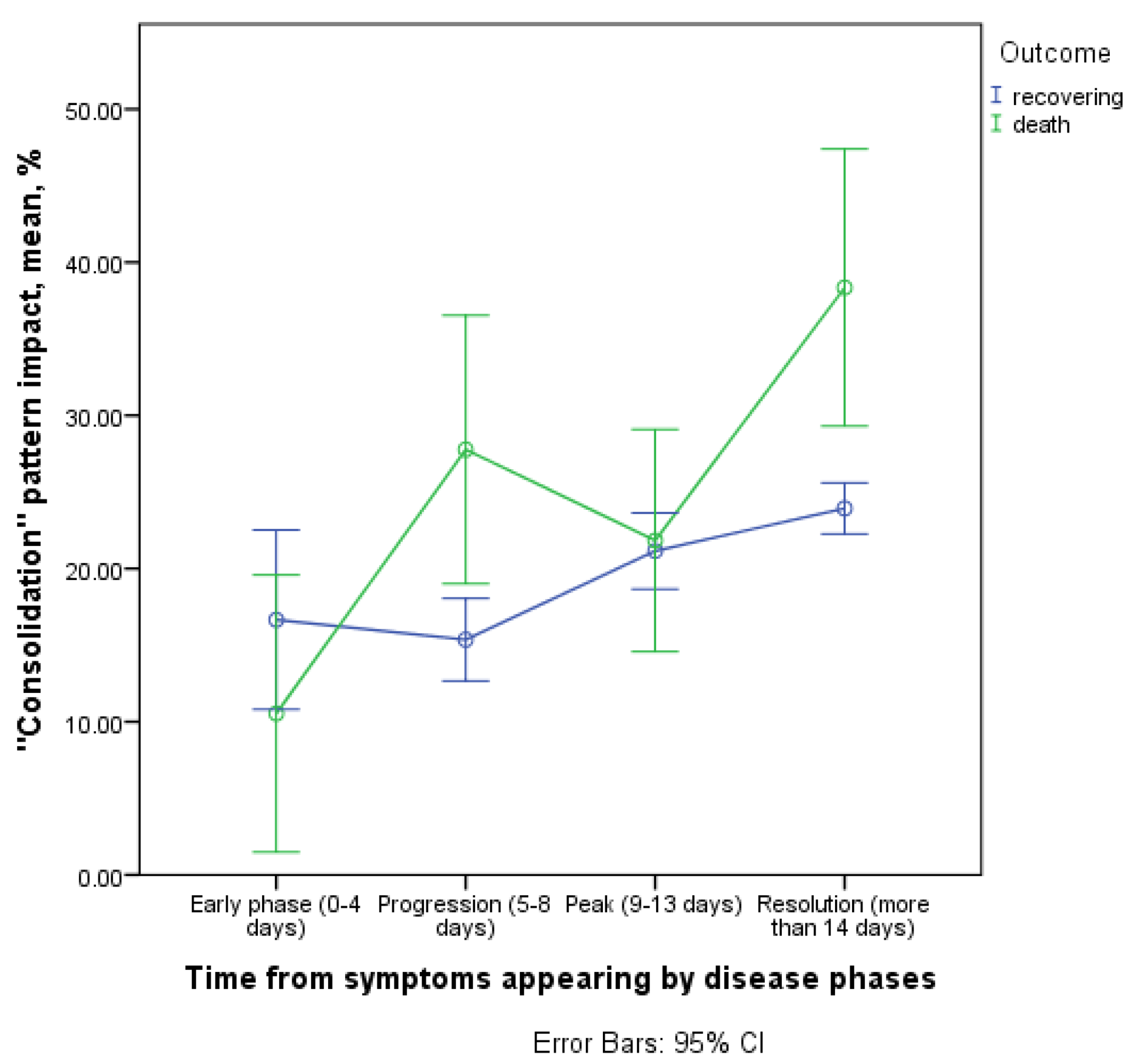
3.3.4. Contribution of the Consolidation Pattern to CT Picture in the Affected Areas
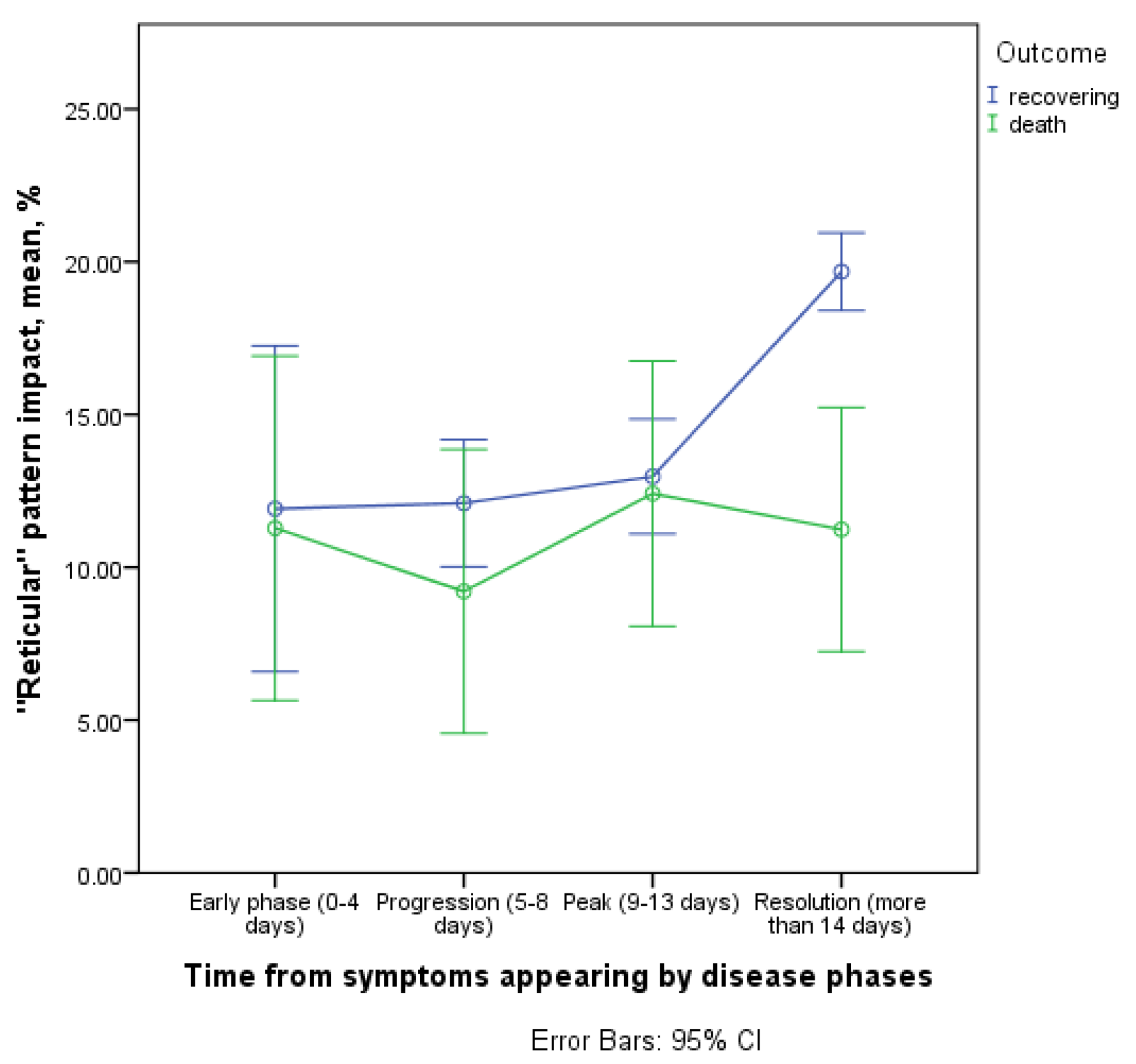
3.3.5. Contribution of Reticular Changes to CT Picture in the Affected Areas
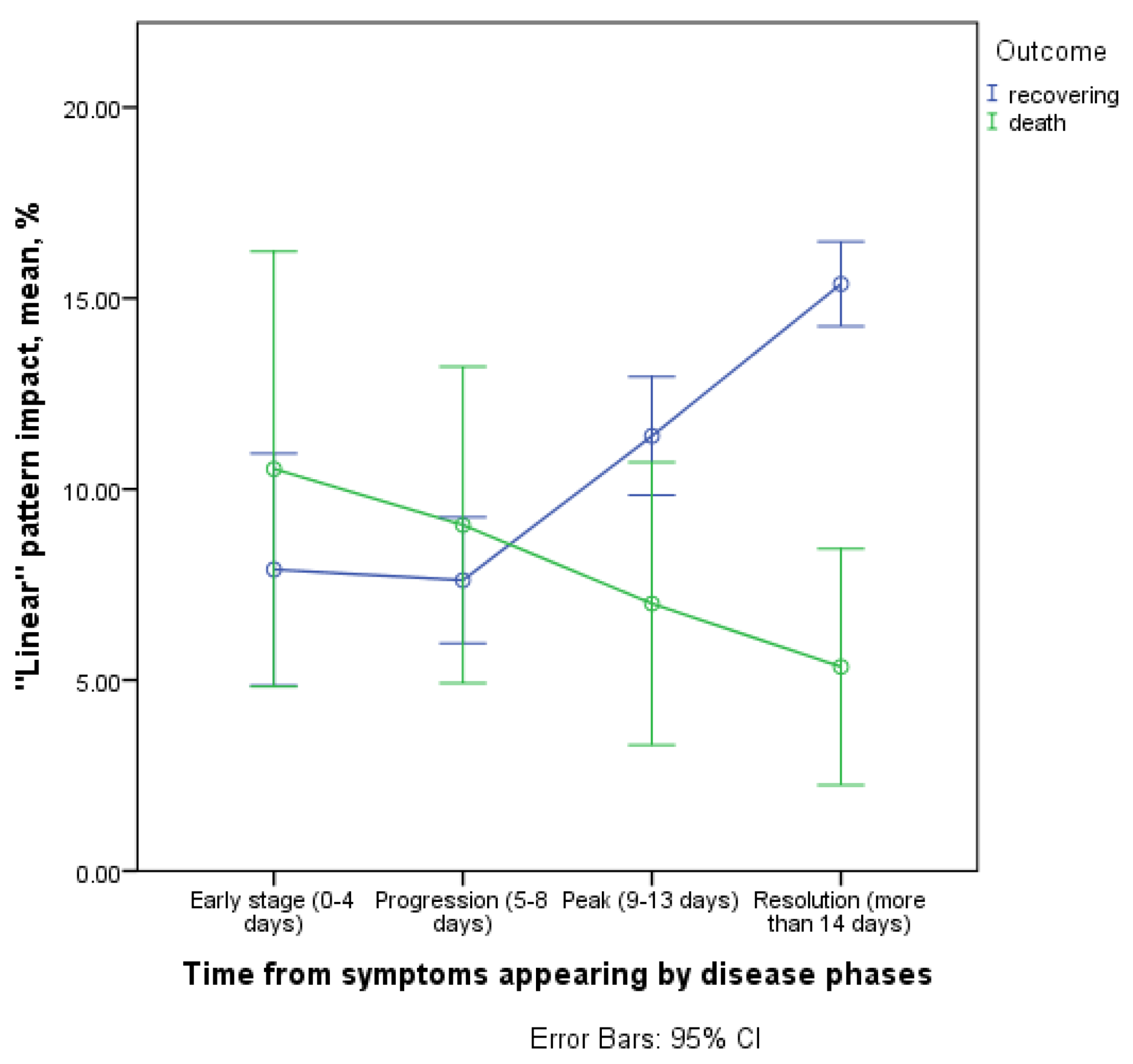
3.3.6. Contribution of Linear Bands to CT Picture in the Affected Areas
3.3.7. Dominant Patterns on Admission Day, Frequency of Pattern Detection
4. Discussion
5. Limitations of Our Study
- Some combinations of radiological patterns were in the ‘gray’ zone, which makes it possible that certain patterns were not registered correctly, as in many other analyzed articles.
- The volume of lung lesion was registered visually, according to scales that are not devoid of shortcomings and subjectivity.
- The sample of fatal cases was relatively small, which reduced the sensitivity of the statistical analysis.
- This study does not include data from pathomorphological studies, which makes our arguments about the mechanisms of development of certain patterns purely hypothetical.
- There may have been a hidden mutual influence of factors (confounding), which may distort the results of our observational study.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 Pathophysiology: A Review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High Expression of ACE2 Receptor of 2019-NCoV on the Epithelial Cells of Oral Mucosa. Int. J. Oral Sci. 2020, 12, 8. [Google Scholar] [CrossRef]
- Wichmann, D.; Sperhake, J.-P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef]
- Black, J.R.M.; Bailey, C.; Przewrocka, J.; Dijkstra, K.K.; Swanton, C. COVID-19: The Case for Health-Care Worker Screening to Prevent Hospital Transmission. Lancet 2020, 395, 1418–1420. [Google Scholar] [CrossRef]
- Li, X.; Ma, X. Acute Respiratory Failure in COVID-19: Is It “Typical” ARDS? Crit. Care 2020, 24, 1–5. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The Incubation Period of Coronavirus Disease 2019 (CoVID-19) from Publicly Reported Confirmed Cases: Estimation and Application. Ann. Intern. Med. 2020, 172, 577–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Zhu, J.; Wang, X.; Yang, J.; Liu, X.F.; Xu, X.K. Characterizing COVID-19 Transmission: Incubation Period, Reproduction Rate, and Multiple-Generation Spreading. Front. Phys. 2021, 8, 1–6. [Google Scholar] [CrossRef]
- van Kampen, J.J.A.; van de Vijver, D.A.M.C.; Fraaij, P.L.A.; Haagmans, B.L.; Lamers, M.M.; Okba, N.; van den Akker, J.P.C.; Endeman, H.; Gommers, D.A.M.P.J.; Cornelissen, J.J.; et al. Duration and Key Determinants of Infectious Virus Shedding in Hospitalized Patients with Coronavirus Disease-2019 (COVID-19). Nat. Commun. 2021, 12, 267. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, L.; Ledda, A.; Wymant, C.; Zhao, L.; Ledda, V.; Abeler, L.; Kendall, M.; Nurtay, A.; Cheng, H.; Ng, T.; et al. The Timing of COVID-19 Transmission. MedRxiv 2020. Preprint. [Google Scholar] [CrossRef]
- Yu, X.; Yang, R. COVID-19 Transmission through Asymptomatic Carriers Is a Challenge to Containment. Influenza Other Respir. Viruses 2020, 14, 474–475. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, J.C.L.; Hare, S.S.; Edey, A.; Devaraj, A.; Jacob, J.; Johnstone, A.; McStay, R.; Nair, A.; Robinson, G. An Update on COVID-19 for the Radiologist—A British Society of Thoracic Imaging Statement. Clin. Radiol. 2020, 75, 323–325. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Chen, X.; Cai, Y.; ** of Italian Echocardiographic Laboratories Activities during the Second Wave of Covid-19 Pandemic and Expectations for the Post-Pandemic Era. J. Clin. Med. 2021, 10, 3466. [Google Scholar] [CrossRef]
- Yang, R.; Li, X.; Liu, H.; Zhen, Y.; Zhang, X.; **. BMC Med. Imaging 2020, 20, 92. [Google Scholar] [CrossRef]
- Liu, X.; Zhou, H.; Zhou, Y.; Wu, X.; Zhao, Y.; Lu, Y.; Tan, W.; Yuan, M.; Ding, X.; Zou, J.; et al. Temporal Radiographic Changes in COVID-19 Patients: Relationship to Disease Severity and Viral Clearance. Sci. Rep. 2020, 10, 10263. [Google Scholar] [CrossRef]
- Zhao, W.; Zhong, Z.; **e, X.; Yu, Q.; Liu, J. Relation Between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. Am. J. Roentgenol. 2020, 214, 1072–1077. [Google Scholar] [CrossRef]
- Zhang, N.; Xu, X.; Zhou, L.-Y.; Chen, G.; Li, Y.; Yin, H.; Sun, Z. Clinical Characteristics and Chest CT Imaging Features of Critically Ill COVID-19 Patients. Eur. Radiol. 2020, 30, 6151–6160. [Google Scholar] [CrossRef]
- McKleroy, W.; Lyn-Kew, K. 500 Million Alveoli from 30,000 Feet: A Brief Primer on Lung Anatomy. Lung Innate Immun. Inflamm. Methods Mol. Biol. 2018, 1809, 3–15. [Google Scholar]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Factor | NR | ND | OR | |
|---|---|---|---|---|
| Gender (m vs. f) | Male | 314 | 37 | 1.97 * (95% CI 1.07–3.62) |
| Female | 268 | 16 | ||
| Gender (m vs. f, aged 59 or more) | Male | 125 | 25 | 1.83 (95% CI 0.92–3.62) |
| Female | 137 | 15 | ||
| Gender (m vs. f, under 59 years old) | Male | 189 | 12 | 8.32 * (95% CI 1.07–64.75) |
| Female | 131 | 1 | ||
| Body mass index | <25 | 124 | 11 | 0.78 (95% CI 0.38–1.60) |
| ≥25 | 420 | 29 | ||
| Body mass index | <30 | 323 | 27 | 0.70 (95% CI 0.36–1.39) |
| ≥30 | 221 | 13 | ||
| Current smoking | Yes | 51 | 5 | 1.17 (95% CI 0.44–3.08) |
| No | 525 | 44 | ||
| Alcohol abuse (self-reported) | Yes | 5 | 3 | 7.13 * (95% CI 1.65–30.72) |
| No | 570 | 48 | ||
| CT-Pattern | Early Phase | Progressive Phase | Peak Phase | Resolution Phase | ||||
|---|---|---|---|---|---|---|---|---|
| %R | %D | %R | %D | %R | %D | %R | %D | |
| Ground glass opacity | 81.8 | 94.4 | 93.1 | 87.0 | 87.3 | 83.3 | 86.1 | 83.8 |
| Crazy paving | 38.7 | 66.7 | 56.0 | 72.7 | 50.2 | 86.7 | 36.3 | 61.8 |
| Consolidations | 48.0 | 47.4 | 56.9 | 87.0 | 67.3 | 76.7 | 71.6 | 91.7 |
| Reticular interstitial changes | 36.5 | 55.6 | 53.0 | 47.8 | 53.8 | 64.5 | 71.1 | 61.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akopyan, G.B.; Berdalin, A.B.; Gubskiy, I.L.; Lelyuk, V.G. Differences in Dynamics of Lung Computed Tomography Patterns between Survivors and Deceased Adult Patients with COVID-19. Diagnostics 2021, 11, 1937. https://doi.org/10.3390/diagnostics11101937
Akopyan GB, Berdalin AB, Gubskiy IL, Lelyuk VG. Differences in Dynamics of Lung Computed Tomography Patterns between Survivors and Deceased Adult Patients with COVID-19. Diagnostics. 2021; 11(10):1937. https://doi.org/10.3390/diagnostics11101937
Chicago/Turabian StyleAkopyan, Gevorg B., Alexander B. Berdalin, Ilya L. Gubskiy, and Vladimir G. Lelyuk. 2021. "Differences in Dynamics of Lung Computed Tomography Patterns between Survivors and Deceased Adult Patients with COVID-19" Diagnostics 11, no. 10: 1937. https://doi.org/10.3390/diagnostics11101937