

Performance of VIDAS® Diagnostic Tests for the Automated Detection of Dengue Virus NS1 Antigen and of Anti-Dengue Virus IgM and IgG Antibodies: A Multicentre, International Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Samples
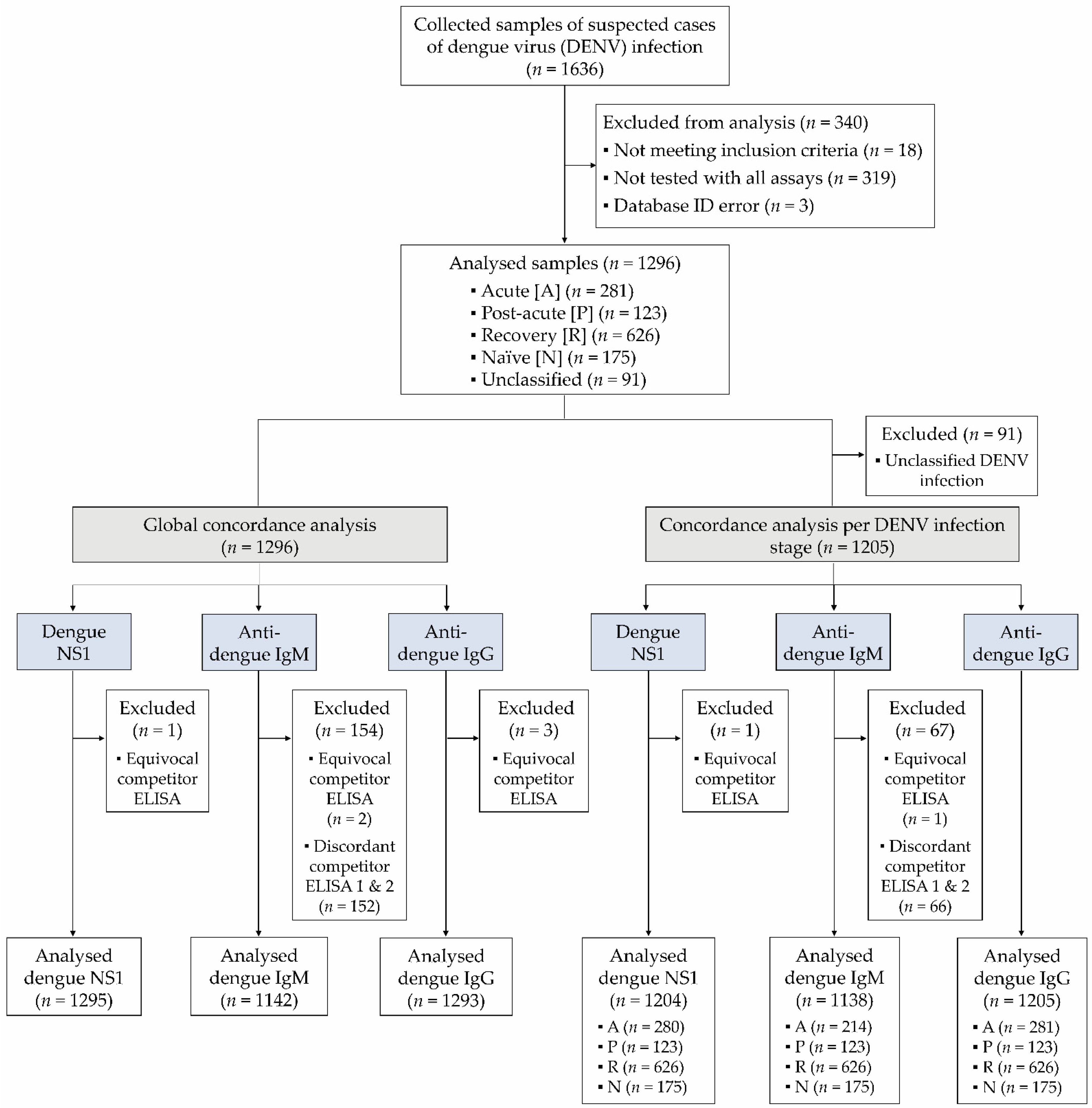
2.2. Study Design and Definitions
2.3. VIDAS® Assays
2.4. Competitor Assays
2.5. Precision Experiments
2.6. Cross-Reactivity Experiments
2.7. Statistical Analyses
3. Results
3.1. Patients’ Characteristics
3.2. VIDAS® Dengue Test Result Description
3.3. Analytical Performance of the VIDAS® Dengue Assays
3.3.1. Assay Precision
3.3.2. Assay Cross-Reactivity
3.4. Clinical Performance of the VIDAS® Dengue Assays
3.4.1. Clinical Sensitivity
3.4.2. Clinical Specificity
3.4.3. Concordance of DENV Infection Classification
3.4.4. Assay Concordance in the Total Study Population and per DENV Infection Stage
3.4.5. Positive Agreement of Combined NS1/IgM and IgM/IgG Tests
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harapan, H.; Michie, A.; Sasmono, R.T.; Imrie, A. Dengue: A Minireview. Viruses 2020, 12, 829. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Ooi, E.-E.; Horstick, O.; Wills, B. Dengue. Lancet 2019, 393, 350–363. [Google Scholar] [CrossRef]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The Global Distribution and Burden of Dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [Green Version]
- Cucunawangsih; Lugito, N.P.H. Trends of Dengue Disease Epidemiology. Virology 2017, 8, 1178122X17695836. [Google Scholar] [CrossRef] [Green Version]
- WHO (Ed.) Dengue: Guidelines for Diagnosis, Treatment, Prevention, and Control; New edition; World Health Organization (WHO) and the Special Programme for Research and Training in Tropical Diseases (TDR): Geneva, Switzerland, 2009; ISBN 978-92-4-154787-1.
- Raafat, N.; Blacksell, S.D.; Maude, R.J. A Review of Dengue Diagnostics and Implications for Surveillance and Control. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 653–660. [Google Scholar] [CrossRef] [Green Version]
- Center for Disease Control and Prevention Testing for Dengue Virus|Dengue|CDC. Available online: https://www.cdc.gov/dengue/healthcare-providers/testing/index.html (accessed on 27 October 2021).
- Pan American Health Organization; World Health Organization. Dengue: Guidelines for Patient Care in the Region of the Americas; PAHO: Washington, DC, USA, 2016; ISBN 978-92-75-31890-4.
- Peeling, R.W.; Artsob, H.; Pelegrino, J.L.; Buchy, P.; Cardosa, M.J.; Devi, S.; Enria, D.A.; Farrar, J.; Gubler, D.J.; Guzman, M.G.; et al. Evaluation of Diagnostic Tests: Dengue. Nat. Rev. Microbiol. 2010, 8, S30–S38. [Google Scholar] [CrossRef] [PubMed]
- Blacksell, S.D.; Jarman, R.G.; Gibbons, R.V.; Tanganuchitcharnchai, A.; Mammen, M.P.; Nisalak, A.; Kalayanarooj, S.; Bailey, M.S.; Premaratna, R.; de Silva, H.J.; et al. Comparison of Seven Commercial Antigen and Antibody Enzyme-Linked Immunosorbent Assays for Detection of Acute Dengue Infection. Clin. Vaccine. Immunol. 2012, 19, 804–810. [Google Scholar] [CrossRef] [Green Version]
- Blacksell, S.D. Commercial Dengue Rapid Diagnostic Tests for Point-of-Care Application: Recent Evaluations and Future Needs? J. Biomed. Biotechnol. 2012, 2012, 151967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blacksell, S.D.; Jarman, R.G.; Bailey, M.S.; Tanganuchitcharnchai, A.; Jenjaroen, K.; Gibbons, R.V.; Paris, D.H.; Premaratna, R.; de Silva, H.J.; Lalloo, D.G.; et al. Evaluation of Six Commercial Point-of-Care Tests for Diagnosis of Acute Dengue Infections: The Need for Combining NS1 Antigen and IgM/IgG Antibody Detection to Achieve Acceptable Levels of Accuracy. Clin. Vaccine Immunol. 2011, 18, 2095–2101. [Google Scholar] [CrossRef] [Green Version]
- Muller, D.A.; Depelsenaire, A.C.I.; Young, P.R. Clinical and Laboratory Diagnosis of Dengue Virus Infection. J. Infect. Dis. 2017, 215, S89–S95. [Google Scholar] [CrossRef] [PubMed]
- Fry, S.R.; Meyer, M.; Semple, M.G.; Simmons, C.P.; Sekaran, S.D.; Huang, J.X.; McElnea, C.; Huang, C.-Y.; Valks, A.; Young, P.R.; et al. The Diagnostic Sensitivity of Dengue Rapid Test Assays Is Significantly Enhanced by Using a Combined Antigen and Antibody Testing Approach. PLoS Negl. Trop. Dis. 2011, 5, e1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pal, S.; Dauner, A.L.; Valks, A.; Forshey, B.M.; Long, K.C.; Thaisomboonsuk, B.; Sierra, G.; Picos, V.; Talmage, S.; Morrison, A.C.; et al. Multicountry Prospective Clinical Evaluation of Two Enzyme-Linked Immunosorbent Assays and Two Rapid Diagnostic Tests for Diagnosing Dengue Fever. J. Clin. Microbiol. 2015, 53, 1092–1102. [Google Scholar] [CrossRef] [Green Version]
- Blessmann, J.; Winkelmann, Y.; Keoviengkhone, L.; Sopraseuth, V.; Kann, S.; Hansen, J.; El Halas, H.; Emmerich, P.; Schmidt-Chanasit, J.; Schmitz, H.; et al. Assessment of Diagnostic and Analytic Performance of the SD Bioline Dengue Duo Test for Dengue Virus (DENV) Infections in an Endemic Area (Savannakhet Province, Lao People’s Democratic Republic). PLoS ONE 2020, 15, e0230337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonnet, C.; Okandze, A.; Matheus, S.; Djossou, F.; Nacher, M.; Mahamat, A. Prospective Evaluation of the SD BIOLINE Dengue Duo Rapid Test during a Dengue Virus Epidemic. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 2441–2447. [Google Scholar] [CrossRef]
- Hunsperger, E.A.; Yoksan, S.; Buchy, P.; Nguyen, V.C.; Sekaran, S.D.; Enria, D.A.; Pelegrino, J.L.; Vázquez, S.; Artsob, H.; Drebot, M.; et al. Evaluation of Commercially Available Anti-Dengue Virus Immunoglobulin M Tests. Emerg. Infect. Dis. 2009, 15, 436–440. [Google Scholar] [CrossRef]
- Pal, S.; Dauner, A.L.; Mitra, I.; Forshey, B.M.; Garcia, P.; Morrison, A.C.; Halsey, E.S.; Kochel, T.J.; Wu, S.-J.L. Evaluation of Dengue NS1 Antigen Rapid Tests and ELISA Kits Using Clinical Samples. PLoS ONE 2014, 9, e113411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaikwad, S.; Sawant, S.S.; Shastri, J.S. Comparison of Nonstructural Protein-1 Antigen Detection by Rapid and Enzyme-Linked Immunosorbent Assay Test and Its Correlation with Polymerase Chain Reaction for Early Diagnosis of Dengue. J. Lab. Physicians 2017, 9, 177–181. [Google Scholar] [CrossRef]
- Lee, H.; Ryu, J.H.; Park, H.S.; Park, K.H.; Bae, H.; Yun, S.; Choi, A.R.; Cho, S.Y.; Park, C.; Lee, D.G.; et al. Comparison of Six Commercial Diagnostic Tests for the Detection of Dengue Virus Non-Structural-1 Antigen and IgM/IgG Antibodies. Ann. Lab. Med. 2019, 39, 566–571. [Google Scholar] [CrossRef] [Green Version]
- Hunsperger, E.A.; Yoksan, S.; Buchy, P.; Nguyen, V.C.; Sekaran, S.D.; Enria, D.A.; Vazquez, S.; Cartozian, E.; Pelegrino, J.L.; Artsob, H.; et al. Evaluation of Commercially Available Diagnostic Tests for the Detection of Dengue Virus NS1 Antigen and Anti-Dengue Virus IgM Antibody. PLoS Negl. Trop. Dis. 2014, 8, e3171. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Li, W.; Wang, J.; Peng, H.; Che, X.; Chen, X.; Zhou, Y. NS1-Based Tests with Diagnostic Utility for Confirming Dengue Infection: A Meta-Analysis. Int. J. Infect. Dis. 2014, 26, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Somlor, S.; Brossault, L.; Grandadam, M. Evaluation of VIDAS® Diagnostic Assay Prototypes Detecting Dengue Virus NS1 Antigen and Anti-Dengue Virus IgM and IgG Antibodies. Diagnostics 2021, 11, 1228. [Google Scholar] [CrossRef] [PubMed]
- Colombo, T.E.; Versiani, A.F.; Dutra, K.R.; Rubiato, J.G.D.; Galvão, T.M.; Negri Reis, A.F.; Nogueira, M.L. Performance of CDC Trioplex QPCR during a Dengue Outbreak in Brazil. J. Clin. Virol. 2019, 121, 104208. [Google Scholar] [CrossRef]
- Johnson, B.W.; Russell, B.J.; Lanciotti, R.S. Serotype-Specific Detection of Dengue Viruses in a Fourplex Real-Time Reverse Transcriptase PCR Assay. J. Clin. Microbiol. 2005, 43, 4977–4983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Combe, M.; Lacoux, X.; Martinez, J.; Méjan, O.; Luciani, F.; Daniel, S. Expression, Refolding and Bio-Structural Analysis of a Tetravalent Recombinant Dengue Envelope Domain III Protein for Serological Diagnosis. Protein. Expr. Purif. 2017, 133, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Clinical & Laboratory Standards Institute EP05-A3: Evaluating Quantitative Measurement Precision, 3rd Edition. Available online: https://clsi.org/standards/products/method-evaluation/documents/ep05/ (accessed on 27 October 2021).
- Clinical & Laboratory Standards Institute EP07: Interference Testing in Clinical Chemistry—Third Edition. Available online: https://clsi.org/standards/products/method-evaluation/documents/ep07/ (accessed on 26 January 2022).
- Clinical & Laboratory Standards Institute EP12-A2: User Protocol for Evaluation of Qualitative Test Performance, 2nd Edition. Available online: https://clsi.org/standards/products/method-evaluation/documents/ep12/ (accessed on 12 October 2022).
- Ambrose, J.H.; Sekaran, S.D.; Azizan, A. Dengue Virus NS1 Protein as a Diagnostic Marker: Commercially Available ELISA and Comparison to QRT-PCR and Serological Diagnostic Assays Currently Used by the State of Florida. J. Trop. Med. 2017, 2017, 8072491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tate, J.; Ward, G. Interferences in Immunoassay. Clin. Biochem. Rev. 2004, 25, 105–120. [Google Scholar]
- Piantadosi, A.; Kanjilal, S. Diagnostic Approach for Arboviral Infections in the United States. J. Clin. Microbiol. 2020, 58, e01926-19. [Google Scholar] [CrossRef]
- Endale, A.; Medhin, G.; Darfiro, K.; Kebede, N.; Legesse, M. Magnitude of Antibody Cross-Reactivity in Medically Important Mosquito-Borne Flaviviruses: A Systematic Review. Infect. Drug. Resist. 2021, 14, 4291–4299. [Google Scholar] [CrossRef] [PubMed]
- Souza, N.C.S.E.; Félix, A.C.; de Paula, A.V.; Levi, J.E.; Pannuti, C.S.; Romano, C.M. Evaluation of Serological Cross-Reactivity between Yellow Fever and Other Flaviviruses. Int. J. Infect. Dis. 2019, 81, 4–5. [Google Scholar] [CrossRef] [Green Version]
- Koraka, P.; Zeller, H.; Niedrig, M.; Osterhaus, A.D.M.E.; Groen, J. Reactivity of Serum Samples from Patients with a Flavivirus Infection Measured by Immunofluorescence Assay and ELISA. Microbes. Infect. 2002, 4, 1209–1215. [Google Scholar] [CrossRef]
- Lustig, Y.; Keler, S.; Kolodny, R.; Ben-Tal, N.; Atias-Varon, D.; Shlush, E.; Gerlic, M.; Munitz, A.; Doolman, R.; Asraf, K.; et al. Potential Antigenic Cross-Reactivity between SARS-CoV-2 and Dengue Viruses. Clin. Infect. Dis. 2021, 73, e2444–e2449. [Google Scholar] [CrossRef]
- Nath, H.; Mallick, A.; Roy, S.; Sukla, S.; Biswas, S. Computational Modelling Supports That Dengue Virus Envelope Antibodies Can Bind to SARS-CoV-2 Receptor Binding Sites: Is Pre-Exposure to Dengue Virus Protective against COVID-19 Severity? Comput. Struct. Biotechnol. J. 2021, 19, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Spinicci, M.; Bartoloni, A.; Mantella, A.; Zammarchi, L.; Rossolini, G.M.; Antonelli, A. Low Risk of Serological Cross-Reactivity between Dengue and COVID-19. Mem. Inst. Oswaldo. Cruz. 2020, 115, e200225. [Google Scholar] [CrossRef] [PubMed]
- Nath, H.; Mallick, A.; Roy, S.; Sukla, S.; Basu, K.; De, A.; Biswas, S. Archived Dengue Serum Samples Produced False-Positive Results in SARS-CoV-2 Lateral Flow-Based Rapid Antibody Tests. J. Med. Microbiol. 2021, 70. [Google Scholar] [CrossRef]
- Vanroye, F.; Bossche, D.V.d.; Brosius, I.; Tack, B.; Esbroeck, M.V.; Jacobs, J. COVID-19 Antibody Detecting Rapid Diagnostic Tests Show High Cross-Reactivity When Challenged with Pre-Pandemic Malaria, Schistosomiasis and Dengue Samples. Diagnostics 2021, 11, 1163. [Google Scholar] [CrossRef]
- Masyeni, S.; Santoso, M.S.; Widyaningsih, P.D.; Asmara, D.W.; Nainu, F.; Harapan, H.; Sasmono, R.T. Serological Cross-Reaction and Coinfection of Dengue and COVID-19 in Asia: Experience from Indonesia. Int. J. Infect. Dis. 2021, 102, 152–154. [Google Scholar] [CrossRef]
- Santoso, M.S.; Masyeni, S.; Haryanto, S.; Yohan, B.; Hibberd, M.L.; Sasmono, R.T. Assessment of Dengue and COVID-19 Antibody Rapid Diagnostic Tests Cross-Reactivity in Indonesia. Virol. J. 2021, 18, 54. [Google Scholar] [CrossRef]
- Khairunisa, S.Q.; Amarullah, I.H.; Churrotin, S.; Fitria, A.L.; Amin, M.; Lusida, M.I.; Soegijanto, S. Potential Misdiagnosis between COVID-19 and Dengue Infection Using Rapid Serological Test. Infect. Dis. Rep. 2021, 13, 540–551. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Ryan, M.; Yohan, B.; Abidin, R.S.; Nainu, F.; Rakib, A.; Jahan, I.; Emran, T.B.; Ullah, I.; Panta, K.; et al. Covid-19 and Dengue: Double Punches for Dengue-Endemic Countries in Asia. Rev. Med. Virol. 2021, 31, e2161. [Google Scholar] [CrossRef]
- Schulte, H.L.; Brito-Sousa, J.D.; Lacerda, M.V.G.; Naves, L.A.; de Gois, E.T.; Fernandes, M.S.; Lima, V.P.; Rassi, C.H.R.E.; de Siracusa, C.C.; Sasaki, L.M.P.; et al. SARS-CoV-2/DENV Co-Infection: A Series of Cases from the Federal District, Midwestern Brazil. BMC Infect. Dis. 2021, 21, 727. [Google Scholar] [CrossRef]
- Mejía-Parra, J.L.; Aguilar-Martinez, S.; Fernández-Mogollón, J.L.; Luna, C.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J.; Díaz-Vélez, C. Characteristics of Patients Coinfected with Severe Acute Respiratory Syndrome Coronavirus 2 and Dengue Virus, Lambayeque, Peru, May-August 2020: A Retrospective Analysis. Travel. Med. Infect. Dis. 2021, 43, 102132. [Google Scholar] [CrossRef] [PubMed]
- Messina, J.P.; Brady, O.J.; Scott, T.W.; Zou, C.; Pigott, D.M.; Duda, K.A.; Bhatt, S.; Katzelnick, L.; Howes, R.E.; Battle, K.E.; et al. Global Spread of Dengue Virus Types: Map** the 70 Year History. Trends Microbiol. 2014, 22, 138–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Site | Collection Site | Samples | Collection Time | Testing Site |
|---|---|---|---|---|
| 1 | Hôpital Sainte Camille & Centre de Recherche Biomoléculaire Pietro Annigoni (CERBA), Ouagadougou, Burkina Faso | Prospective cohort Adults and children | June 2020–October 2020 | Institut de Recherche en Sciences de la Santé (IRSS), Ouagadougou, Burkina Faso |
| 2 | Centro Integrado de Pesquisa, Hospital de Base, São José do Rio Preto, Brazil | Retrospective & prospective cohorts 1 Adults | February 2019–August 2020 | Laboratório de Pesquisas em Virologia, FAMERP, São José do Rio Preto, Brazil |
| 3 | India, Vietnam, The Philippines, Peru, Honduras, and Dominican Republic | Retrospective cohort 2 Adults and children | September 2015–September 2020 | Clinical Affairs Laboratory, bioMérieux, Marcy l’Etoile, France |
| Competitor ELISA | Name of Assay | Provider |
|---|---|---|
| NS1 1 | Dengue NS1 Antigen DxSelect™ (EL1510; IfU Rev. C) | Focus Diagnostics, DiaSorin Molecular LLC, Cypress, CA, USA |
| DENV DetectTM NS1 ELISA (DNS1-1; IfU No. 900109-02) | InBios International, Inc., Seattle, Washington, DC, USA | |
| IgM 2 | Panbio Dengue IgM Capture ELISA (01PE20) | Abbott Laboratories, Abbott Park, IL, USA |
| DENV Detect IgM Capture ELISA (DDMS-1) | InBios International, Inc., Seattle, Washington, DC, USA | |
| IgG | Panbio Dengue IgG Indirect ELISA (01PE30) | Abbott Laboratories, Abbott Park, IL, USA |
| Stage of DENV Infection | RT-PCR and/or NS1 Competitor ELISA Result 1 | IgM Competitor ELISA Results 2 | IgG Competitor ELISA Result 3 |
|---|---|---|---|
| Naïve 8 | Negative 4 | Negative | Negative |
| Acute | Positive 5 | Positive or negative | Positive or negative |
| Post-Acute | Negative 4 | Positive | Positive |
| Recovery | Negative 4 | Negative | Positive |
| Unclassified | Negative 4 or Undetermined 6 | Positive or Undetermined 7 | Negative or Undetermined 6 |
| Study Population, N (%) | 1296 (100.0%) |
|---|---|
| Study population according to the testing site, N (%) Site 1 (Burkina Faso; sample collection and testing) Site 2 (Brazil; sample collection and testing) Site 3 (France; externally acquired sample testing) | 480 (37.0%) 392 (30.3%) 424 (32.7%) |
| Age in years, median (range) | 32.0 (5–88) |
| Sex, N (%) Female Male | 741 (57.2%) 555 (42.8%) |
| RT-PCR-positive samples, N (%) | 154 (11.9%) |
| Serotype distribution among RT-PCR-positive samples, N (%) DENV-1 DENV-2 DENV-3 DENV-4 | 74/154 (48.0%) 72/154 (46.8%) 6/154 (3.9%) 2/154 (1.3%) |
| Sample distribution according to time from symptom onset, N (%) 0–3 days 4–5 days 6–8 days 9–15 days 16 days–1 month >1 month Unknown | 477 (36.8%) 228 (17.6%) 456 (35.2%) 78 (6.0%) 34 (2.6%) 16 (1.2%) 7 (0.6%) |
| DENV infection stage 1, N (%) Acute Post-Acute Recovery Naïve Unclassified | 281 (21.7%) 123 (9.5%) 626 (48.3%) 175 (13.5%) 91 (7.0%) |
| VIDAS® Dengue Assay | Sample | Total Number of Measurements | Mean Index | Repeatability (within-Run Precision) | Within-Laboratory Precision 2 | ||
|---|---|---|---|---|---|---|---|
| SD | CV (%) | SD | CV (%) | ||||
| NS1 | A (negative, high) | 79 1 | 0.62 | 0.05 | 7.5 | 0.05 | 8.2 |
| B (positive, low) | 80 | 1.26 | 0.06 | 5.1 | 0.07 | 5.4 | |
| C (positive, moderate) | 80 | 1.71 | 0.07 | 4.1 | 0.08 | 4.9 | |
| IgM | A (negative, high) | 80 | 0.82 | 0.02 | 3.0 | 0.09 | 10.7 |
| B (positive, low) | 80 | 1.16 | 0.03 | 2.7 | 0.09 | 8.1 | |
| C (positive, moderate) | 80 | 1.56 | 0.03 | 1.8 | 0.11 | 7.2 | |
| IgG | A (negative, high) | 80 | 0.73 | 0.03 | 4.4 | 0.04 | 5.8 |
| B (positive, low) | 80 | 1.28 | 0.05 | 4.1 | 0.07 | 5.7 | |
| C (positive, moderate) | 80 | 1.44 | 0.07 | 4.5 | 0.09 | 6.4 | |
| Potentially Interfering Infections | Proportion of Cross-Reactions with VIDAS® Dengue Assays | ||
|---|---|---|---|
| NS1 | IgM | IgG | |
| Herpes simplex virus (HSV1/2) | 0/6 1 | 2/13 | 3/14 |
| Varicella zoster virus (VZV) | 0/3 1 | 4/15 | 0/10 |
| Cytomegalovirus (CMV) | 0/3 1 | 4/17 | 0/10 |
| Epstein-Barr virus (EBV) | 0/3 1 | 3/14 | 2/15 |
| Influenza virus (IAV/IBV) | Nd | 2/11 | 2/10 |
| Borrelia burgdorferi | Nd | 2/14 | nd |
| Plasmodium falciparum | 0/3 1 | 3/10 | 0/10 |
| Leptospira | Nd | 3/12 | nd |
| Chikungunya virus (CHIKV) | 0/3 1 | 0/13 | 0/7 |
| West Nile virus (WNV) | 0/3 1 | 1/18 | 2/9 |
| Yellow fever virus (YFV) | 0/3 1 | 2/21 | 0/14 |
| Zika virus (ZIKV) | 0/3 1 | 1/14 | 0/8 |
| Hepatitis A virus (HAV) | Nd | 1/15 | nd |
| Hepatitis B virus (HBV) | 0/10 | 2/14 | 0/7 |
| Hepatitis C Virus (HCV) | 1/9 | 3/14 | 1/14 |
| Parvovirus B19 | Nd | 4/14 | 0/10 |
| Human immunodeficiency virus (HIV) | Nd | 1/14 | 2/9 |
| HIV P24 antigen | 0/9 | nd | nd |
| Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) | 0/10 | 2/16 | 1/20 |
| Total (%) | 1/68 (1.5%) | 40/259 (15.4%) | 13/167 (7.8%) |
| Reference Test | Population | VIDAS® NS1 | NS1 ELISA 2 | ||
|---|---|---|---|---|---|
| n/N 1 | % [95% CI] | n/N 1 | % [95% CI] | ||
| RT-PCR | All acute samples | 98/153 | 64.1% [56.2–71.2] | 102/153 | 66.7% [58.9–73.6] |
| D0-5 acute samples | 81/106 | 76.4% [67.5–83.5] | 82/106 | 77.4% [68.5–84.3] | |
| Population | VIDAS® NS1 | VIDAS® IgM | VIDAS® IgG | |||
|---|---|---|---|---|---|---|
| n/N 1 | % [95% CI] | n/N 1 | % [95% CI] | n/N 1 | % [95% CI] | |
| Naïve samples 2 | 175/175 | 100.0% [97.9–100.0] | 152/175 | 86.9% [81.1–91.1] | 156/175 | 89.1% [83.7–92.9] |
| Stage of DENV Infection 2 | Agreement | |
|---|---|---|
| n/N 1 | % [95% CI] | |
| Acute (all) | 249/281 | 88.6% [84.4–91.8] |
| Acute (D0-5) | 156/163 | 95.7% [91.4–98.3] |
| Post-Acute | 78/123 | 63.4% [54.6–71.4] |
| Recovery | 430/626 | 68.7% [65.0–72.2] |
| Naïve | 142/175 | 81.1% [74.7–86.2] |
| Unclassified | 2/91 | 2.2% [0.3–7.7] |
| VIDAS® Dengue Assay | Population | Positive Agreement | Negative Agreement | Overall Agreement | |||
|---|---|---|---|---|---|---|---|
| n/N 1 | % [95% CI] | n/N 1 | % [95% CI] | n/N 1 | % [95% CI] | ||
| NS1 | Total | 191/229 | 83.4% [78.0–87.7] | 1058/1066 | 99.2% [98.5–99.7] | 1249/1295 | 96.4% [95.3–97.4] |
| Acute (all) | 191/229 | 83.4% [78.0–87.7] | 49/51 | 96.1% [86.5–99.5] | 240/280 | 85.7% [81.1–89.3] | |
| Acute (D0-5) | 128/138 | 92.8% [87.2–96.0] | 22/24 | 91.7% [74.2–97.7] | 150/162 | 92.6% [87.5–95.7] | |
| Post-Acute | N/A | - | 123/123 | 100.0% [97.0–100.0] | N/A | - | |
| Recovery | N/A | - | 621/626 | 99.2% [98.1–99.7] | N/A | - | |
| IgM | Total | 213/266 | 80.1% [74.9–84.4] | 689/876 | 78.7% [75.8–81.2] | 902/1142 | 79.0% [76.5–81.2] |
| Acute (all) | 120/142 | 84.5% [77.7–89.5] | 57/72 | 79.2% [68.4–86.9] | 177/214 | 82.7% [77.1–87.2] | |
| Acute (D0-5) | 65/74 | 87.8% [78.5–93.5] | 34/45 | 75.6% [61.3–85.8] | 99/119 | 83.2% [75.5–88.8] | |
| Post-Acute | 92/123 | 74.8% [66.5–81.6] | N/A | - | N/A | - | |
| Recovery | N/A | - | 477/626 | 76.2% [72.7–79.4] | N/A | - | |
| IgG | Total | 940/1096 | 85.8% [83.6–87.7] | 170/197 | 86.3% [80.8–90.4] | 1110/1293 | 85.8% [83.8–87.6] |
| Acute (all) | 195/264 | 73.9% [68.2–78.8] | 10/17 | 58.8% [36.0–78.4] | 205/281 | 73.0% [67.5–77.8] | |
| Acute (D0-5) | 129/153 | 84.3% [77.7–89.2] | 4/10 | 40.0% [16.8–68.7] | 133/163 | 81.6% [74.9–86.8] | |
| Post-Acute | 99/123 | 80.5% [72.6–86.5] | N/A | - | N/A | - | |
| Recovery | 567/626 | 90.6% [88.0–92.6] | N/A | - | N/A | - | |
| VIDAS® Dengue Assay | Population | Positive Agreement | |
|---|---|---|---|
| n/N 1 | % [95% CI] | ||
| NS1/IgM 2 | Total | 316/362 | 87.3% [83.5–90.3] |
| Total (D0-5) | 145/152 | 95.4% [90.7–98.1] | |
| Acute (all) | 223/238 | 93.7% [89.9–96.1] | |
| Acute (D0-5) | 134/139 | 96.4% [91.8–98.8] | |
| IgM/IgG 3 | Total | 1011/1100 | 91.9% [90.1–93.4] |
| Post-Acute | 113/123 | 91.9% [85.7–95.5] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Versiani, A.F.; Kaboré, A.; Brossault, L.; Dromenq, L.; dos Santos, T.M.I.L.; Milhim, B.H.G.A.; Estofolete, C.F.; Cissé, A.; Sorgho, P.A.; Senot, F.; et al. Performance of VIDAS® Diagnostic Tests for the Automated Detection of Dengue Virus NS1 Antigen and of Anti-Dengue Virus IgM and IgG Antibodies: A Multicentre, International Study. Diagnostics 2023, 13, 1137. https://doi.org/10.3390/diagnostics13061137
Versiani AF, Kaboré A, Brossault L, Dromenq L, dos Santos TMIL, Milhim BHGA, Estofolete CF, Cissé A, Sorgho PA, Senot F, et al. Performance of VIDAS® Diagnostic Tests for the Automated Detection of Dengue Virus NS1 Antigen and of Anti-Dengue Virus IgM and IgG Antibodies: A Multicentre, International Study. Diagnostics. 2023; 13(6):1137. https://doi.org/10.3390/diagnostics13061137
Chicago/Turabian StyleVersiani, Alice F., Antoinette Kaboré, Ludovic Brossault, Loïc Dromenq, Thayza M. I. L. dos Santos, Bruno H. G. A. Milhim, Cássia F. Estofolete, Assana Cissé, Pegdwendé Abel Sorgho, Florence Senot, and et al. 2023. "Performance of VIDAS® Diagnostic Tests for the Automated Detection of Dengue Virus NS1 Antigen and of Anti-Dengue Virus IgM and IgG Antibodies: A Multicentre, International Study" Diagnostics 13, no. 6: 1137. https://doi.org/10.3390/diagnostics13061137