1. Introduction
Among chronic metabolic diseases with a high incidence and mortality, diabetes is one of the most widely recognized public health issues nowadays [
1]. Statistics from the International Diabetes Federation reveal that the world developed 463 million new diabetes cases in 2019, and this figure is expected to rise to 700.2 million by 2045, with diabetes-related costs accounting for 12% of global healthcare consumption [
2]. As the incidence of diabetes increases, the incidence of complications increases accordingly [
3], with diabetic peripheral neuropathy (DPN) being one of the most common complications. As a neuropathy caused by chronic hyperglycemia [
4,
5], DPN is widely regarded as a major hazardous factor for foot ulcers and even lower limb amputations, and has an extremely high rate of disability and mortality, and a risk of death which even exceeds that of some cancers, for example, breast carcinoma and prostate adenocarcinoma [
6]. Furthermore, the pathogenesis of DPN is exceptionally intricate, including multiple pathophysiological processes such as chronic inflammatory response [
7], neurotrophic disorders [
8], and oxidative stress [
9], which cause DPN under the combined action of multiple variables. Unfortunately, there is no effective treatment for DPN in the medical community up to date. However, clinical symptoms in the early stages of DPN lack specificity, and the majority of patients have irreversible pathological changes in the peripheral nerves once symptoms such as limb numbness and pain occur [
10]. Therefore, early diagnosis of this symptom remains a challenge in clinical practice.
Vitamin D is a fat-soluble hormone. Vitamin D deficiency is closely related to diabetic microangiopathy, and studies [
11] have highlighted that vitamin D deficiency might be a critical cause of DNP. Moreover, numerous findings have shown that vitamin D deficiency has a significant impact on patients with DPN. Adverse conditions will increase the prevalence of DPN, leading to foot ulcers, lower limb amputations, and even death [
6,
11,
12]. Since DPN is an irreversible disease, it is imperative to predict the likelihood of DPN, using serum 25 hydroxyvitamin D3 [25(OH)D3] (vitamin D in vivo in the form of 25(OH)D3) and associated risk factors, until type 2 diabetes mellitus (T2DM) has been identified as DPN. However, there have been few reports of correlation between the 25(OH)D3 factor and DPN, and there has never been an unprecedented risk prediction model based on 25(OH)D3 to predict the occurrence of DPN.
As a straightforward statistical visualization tool, nomograms have been broadly utilized in recent years to foresee the generation, development, prognosis, and endurance of diseases [
13,
14]. This study aims to establish a nomogram prediction model. The model incorporates a series of hazard factors for early prediction while aiding high-risk populaces to initiate timely interventions to diminish morbidity and mortality from diabetic peripheral neuropathy.
4. Discussion
Diabetic peripheral neuropathy is one of the most common complications of diabetes. The International Diabetes League [
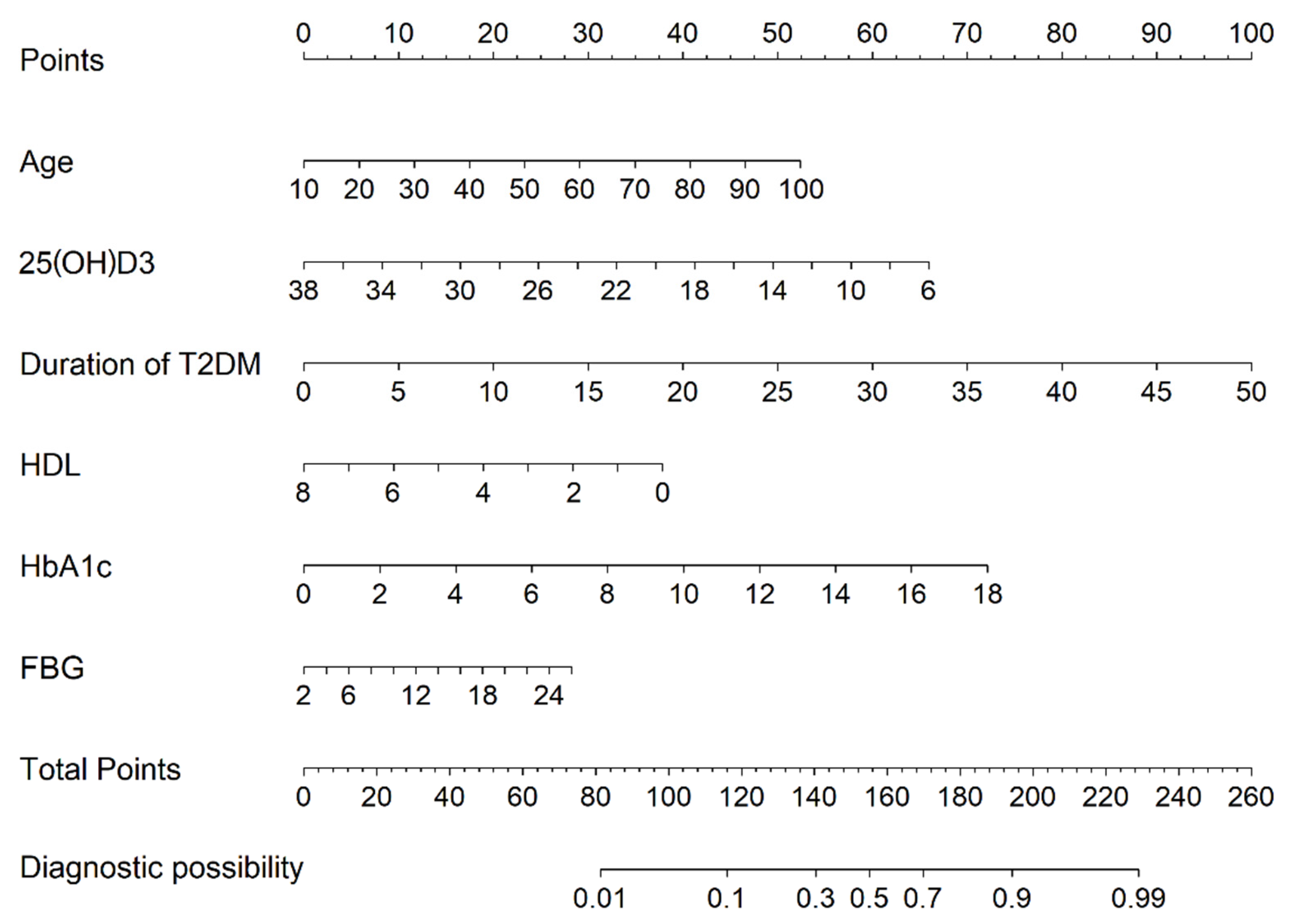
2] survey revealed that the incidence of diabetic peripheral neuropathy is essentially as high as 30% to 50%. Additionally, once a diabetic patient develops neuropathy, the 5–10-year mortality rate is as high as 25% to 50%. Previous studies have reported the related factors of PDN, such as course of disease: hyperglycemia and hyperlipidemia, but a complete and comprehensive risk model for DPN assessment is still lacking. Our study is the first to include 25(OH)D3 in a risk prediction model to assess the risk of develo** DPN in type 2 diabetes mellitus in China. The prediction model included six clinically available parameters, and the results showed that Age, 25(OH)D3, Duration of T2DM, HDL, HbA1c, and FBG were risk factors for DPN in T2DM. Additionally, the model will assist clinicians to identify high-risk individuals at an early stage and to apply appropriate interventions to improve the prognosis for T2DM.
In recent years, the relationship between vitamin D and microvascular complications of type 2 diabetes has attracted increasing attention from scholars at home and abroad. DPN is one of the main microvascular complications of diabetes. However, there is relatively little existing research available on the association of vitamin D with DPN. A retrospective study [
20] comparing vitamin D deficiency and DPN in T2DM included 87 patients with DPN and 123 patients without DPN. The results found that the serum 25 (OH) D3 concentration in the DPN group was significantly lower than that in the DPN-free group. A total of 81% of patients in the DPN group suffered from vitamin D deficiency while 60.4% of the non-DPN group had a vitamin D deficiency. A similar cross-sectional study [
11] discovered that the prevalence of DPN was comparable in the vitamin D-deficient and vitamin D-sufficient groups (31.89% vs. 31.80%). However, the prevalence of DPN increased to 46.63% in the vitamin D-deficient group. A case-control study conducted by Halawa M R et al. [
21] in 178 prediabetic patients in Egypt demonstrated that vitamin D levels were inversely correlated with peripheral neuropathy severity (r = −0.47,
p < 0.001). Unexpectedly, after vitamin D supplementation, the neuropathy score dropped from (Mean = 6.4, SD = 1.6) to (Mean = 2.5, SD = 0.9). In this study, vitamin deficiency and DPN correlation showed a strong significance, which is consistent with existing research. The most likely reason for this is that vitamins can promote the secretion of pancreatic B cells, reduce insulin resistance by increasing insulin secretion, improve blood sugar in patients, and protect the central nervous system to a certain extent. Dou X et al. [
22] confirmed through animal experiments that 25(OH)D3 has a protective effect on the nerves of diabetic rats, while another animal experiment [
23] demonstrated that the level of nerve growth factor in rats after the treatment of diabetic neuropathy with vitamin D3 derivatives was increased, suggesting that vitamin D can act on various cells of the nervous system and exert neuroprotective effects by regulating calcium homeostasis in neuronal cells. Meanwhile, a strong correlation between pro-inflammatory factors and DPN was found in the results of a 5-year prospective study in China [
24], which was confirmed in a national health and nutrition examination survey study in the United States [
25]. The researchers found that vitamin D can downregulate the expression of inflammatory factors such as tumor necrosis factor α (TNF-α), interleukin-6 (IL-6), and interleukin-1 receptor antagonist (IL-1RA), and can also inhibit the occurrence and development of inflammatory response, and thus can inhibit the occurrence of DPN. This imposes a requirement that in the future health management of DPN patients, attention should be paid to the monitoring of serum 25(OH)D3 and appropriate supplementation of vitamin D should be given. This requirement is expected to be one of the therapeutic means of preventing DPN and even accelerate the recovery of patients.
In most epidemiological studies of DPN, age and the course of diabetes are the most frequently evaluated immutable hazardous factors [
3,
26,
27]. In a study of 60 hospitalized T2DM [
28], the incidence of DPN in patients aged 20 to 34 years, 35 to 49 years, 50 to 64 years, and ≥ 65 years was found to be 8.4%, 22.7%, 33.0%, and 42.4%, respectively, and the incidence of DPN was significantly different from that of age. Studies by Popesco et al. [
29] have shown a DPN prevalence of 28.8% based on the Michigan Neuropathy Screening Scale (MNSI) score, which is significantly positively associated with higher age. On the other hand, Skalli et al. [
30] conducted a cross-sectional study of 111 T2DM, and subgroup analysis discovered that in patients with DPN, the older they were, the lower the 25(OH)D3 level. This conclusion was confirmed in a cross-sectional study of older patient populations in Shanghai [
31]. The results of the study showed that vitamin D deficiency is prevalent in elderly T2DM, which also proves the presence of age-affected DPN. Chia-Tung et al. [
32] and Zhang et al. [
33] found that the longer the course of diabetes, the higher the prevalence of DPN, and it may be that neurofibropathy in patients with DPN leads to a decrease in fibrous nerve density, deepening the degree of skin denexylation and thus increasing the risk of DPN. Additionally, in a three-year follow-up study [
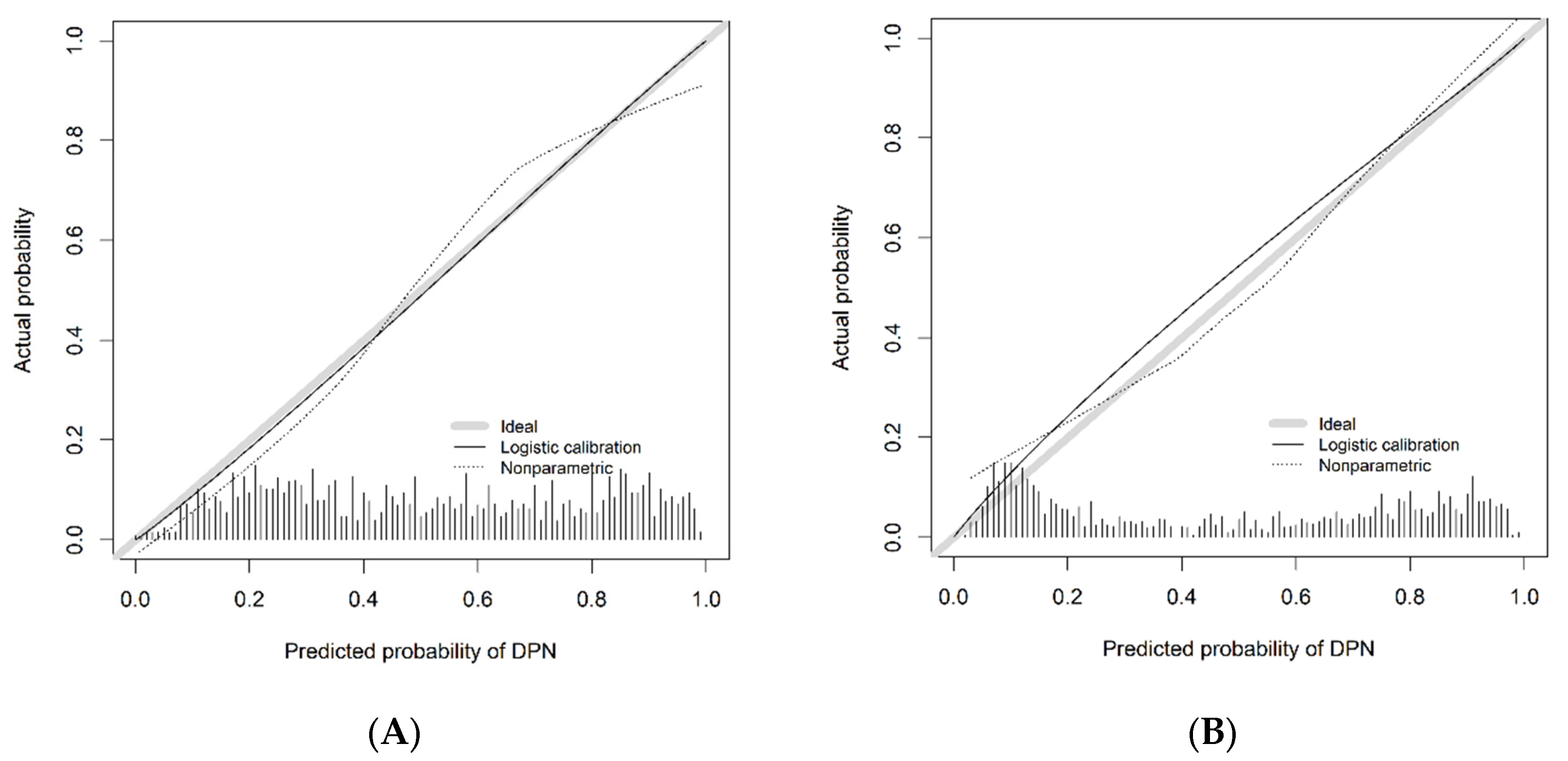
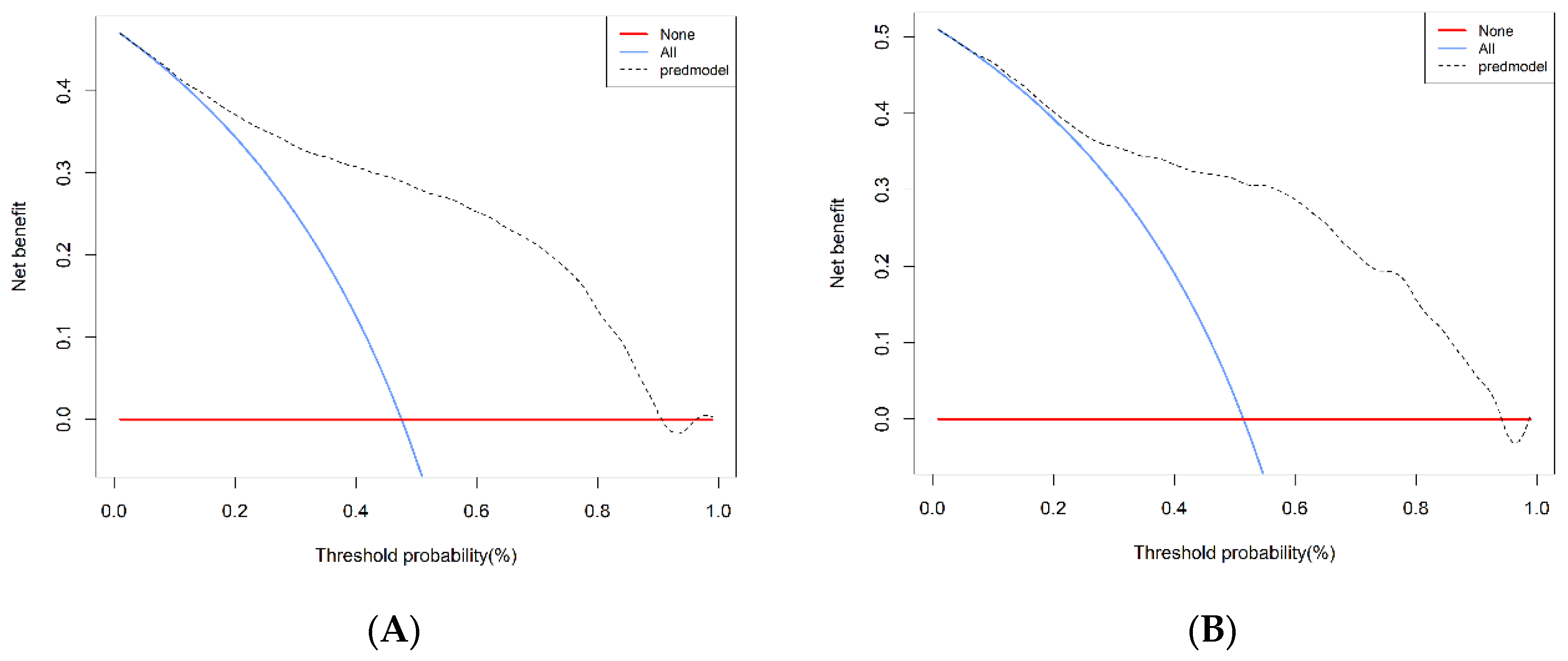
34] in the Shihezi community in ** DPN in T2DM using 25(OH)D3 as the major component. The external validation confirmed that the model is extremely accurate and displays favorable consistency, which can assist in early clinical intervention, and may be of substantial significance in diminishing the prevalence of and mortality from DPN in the future.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}