1. Introduction
In recent years, technological advancements such as next-generation sequencing (NGS) have facilitated numerous studies examining the relationship between systemic diseases and the microbiome [
1]. The oral cavity and gut are significant microbial habitats and have a crucial role in diseases related to the microbiome [
2]. The oral cavity has the second-highest biomass after the gut. According to the Human Oral Microbiome Database (HOMD), there are approximately 770 bacterial species reported, of which only 58% have been officially named. It is still uncharted territory with a wide variety of species that are unnamed but cultivated and known only as uncultivated phylotypes (eHOMD version 3.1;
www.homd.org). The oral cavity contains various microbial habitats, including the buccal mucosa, subgingival plaque, supragingival plaque, palate, saliva, tonsils, tongue, and throat [
3]. Saliva is a non-invasive and easily obtained diagnostic sample that can influence other microbiomes, particularly the gut microbiome [
3]. Therefore, it is natural to use saliva samples to study the oral microbiome. However, the lack of standardized saliva collection methods has hindered the use of saliva in microbiome research. Lim, Yenkai, et al. [
4] found that saliva sample collection methods do not significantly influence salivary microbiome profiles. The human oral microbiome plays a crucial role in protecting the body from external pathogens through proper interactions [
5]. However, disruption of the oral microbiome can lead to various oral diseases, including periodontitis, dental caries, and oral mucosal diseases, as well as non-oral diseases such as rheumatoid arthritis, cancer, and diabetes [
6,
7,
8]. Most of the association between the oral microbiome and oral disease is focused on periodontitis. Systemic autoimmune diseases such as RA, systemic lupus erythematosus (SLE), and primary Sjogren’s syndrome (SS) have been studied. Among these, RA patients had higher disease activity with higher serum antibodies to
Porphyromonas gingivalis, an oral anaerobic bacterium involved in the pathogenesis of periodontitis [
9]. Patients with SLE have increased bacteria in the periodontal area compared to controls [
10] and periodontal disease has also been associated with SLE, increasing the risk or severity of SLE [
11]. Reduced salivation is the most important factor in altering the oral microbiome, but the role of the oral microbiome in the pathogenesis of SS remains unclear [
8]. Among oral autoimmune diseases, there are a few studies on oral lichen planus (OLP).
OLP represents a chronic inflammatory disorder affecting the oral mucosa, typically observed in women over the age of 50 [
12]. It is T cell-mediated, with the pathogenesis characterized by an exaggerated immune response of T cells to specific antigens. Nevertheless, the precise antigens triggering OLP development remain elusive. Although various factors such as systemic medications, viral infections, and dental restoration materials have been proposed as contributors, their exact roles in OLP development remain incompletely understood [
13,
14]. Active research persists in identifying diverse antigens and elucidating the connection between the oral microbiome and OLP [
15].
There are several types of OLP, including reticular, plaque, atrophic, papular, erosive, and bullous [
12]. The two primary types of OLP are non-erosive (NE) and erosive (E) OLP. Asymptomatic patients with typical NE-OLP are often left untreated and only require follow-up checks. However, E-OLP must be treated, as it can cause pain and bleeding, making it difficult for patients to maintain good oral hygiene and leading to secondary infections [
16]. Wang, H. et al. [
17] reported a higher presence of Th17 cells in E-OLP compared to NE-OLP, while Shiva et al. [
18] found an increase in p53 expression, which can serve as a biomarker for cancer, in E-OLP. Although there are studies on the clinical, histological, and immune response differences between E-OLP and NE-OLP, there is a lack of research on the specific differences that lead to the development of NE versus E forms of OLP [
16,
19,
20,
21].
Therefore, the study of OLP and the host’s oral microbiome profile using NGS may provide new insights into the pathogenesis of OLP. However, a very limited number of studies have been conducted on various samples, including buccal mucosa swabs, subgingival plaque, and unstimulated saliva samples with small sample sizes, resulting in inconsistent results [
15]. Research on the relationship between the oral microbiome and OLP is still in its early stages. Hence, the aim of this study is to compare the microbial profiles between OLP patients and healthy controls (HC), as well as between NE-OLP and E-OLP patients, using unstimulated saliva samples.
4. Discussion
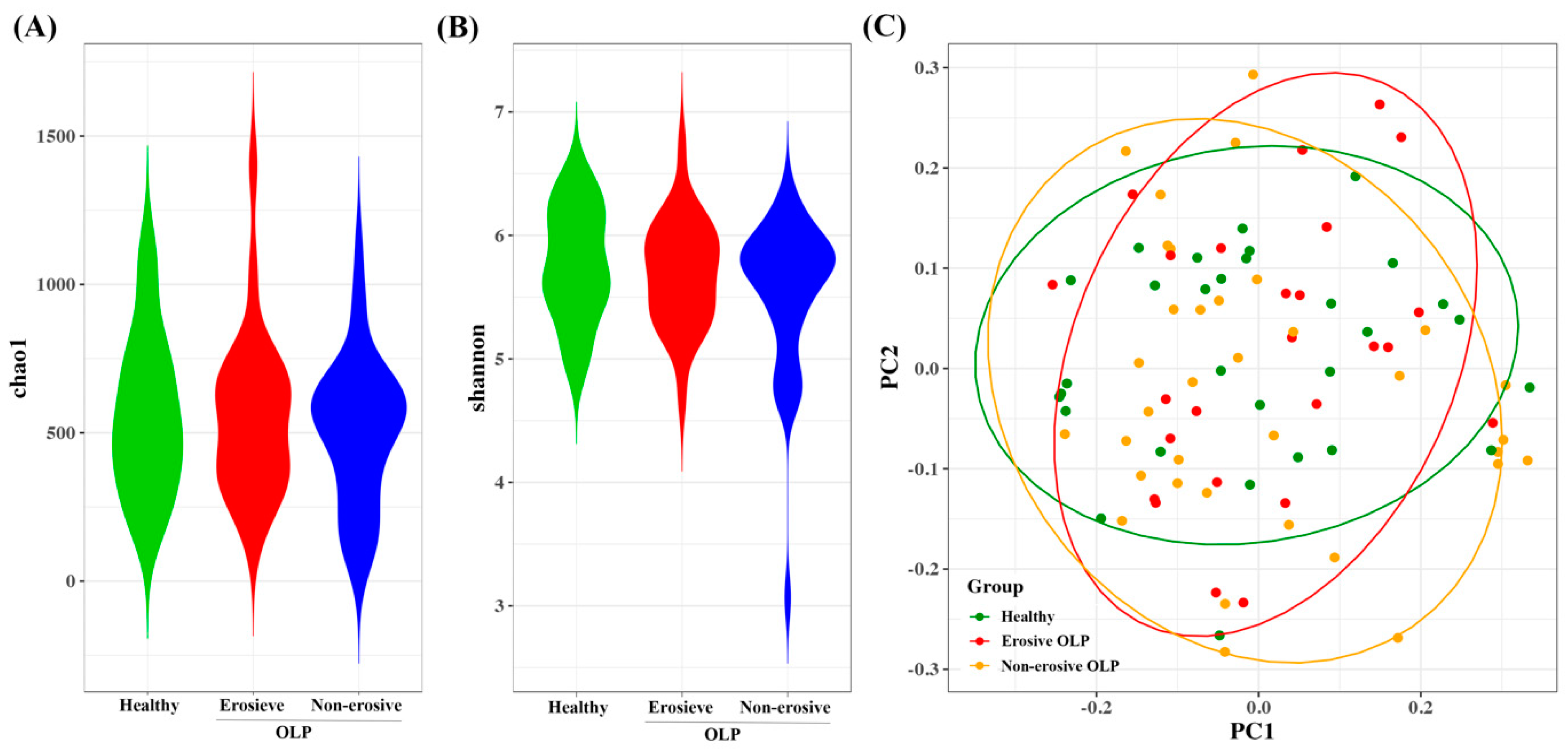
This study aimed to investigate the microbial community in the saliva of patients with OLP, both with and without erosive lesions, and compare it to that of HC. In this study, the results showed that there was no difference in bacterial species diversity between OLP and HC, but there was a difference in composition (
Figure 1). Consistent with previous studies, there were no statistically significant differences in bacterial alpha diversity between the three groups, as measured by the Chao1 and Shannon indices [
26,
27]. Beta diversity did not differ between the OLP groups, but it did differ between E-OLP and NE-OLP compared to HC. Yu et al. [
28] showed a difference in beta diversity between E-OLPs and NE-OLPs, whereas Wang et al. [
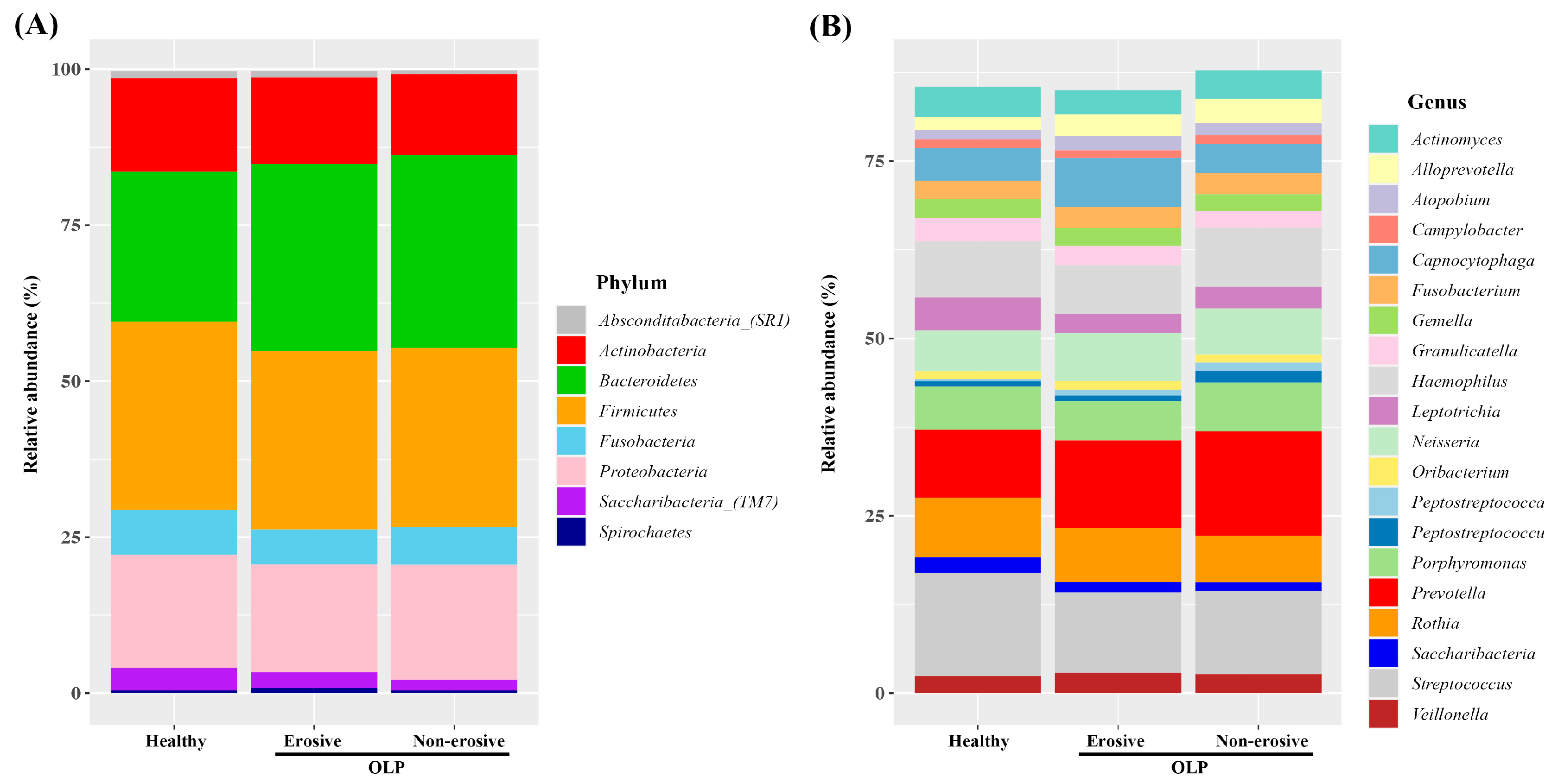
27] found no such difference, which is consistent with the results of this study. This discrepancy may be attributed to differences in primer selection in sequencing methods, bioinformatic analysis methods, and the number of subjects included in the studies. At the phylum level, the most commonly observed bacteria are Firmicutes, Bacteroidetes, Proteobacteria, Actinobacteria, and Fusobacteria. These findings are consistent with previous research [
29,
30,
31]. While there was variation in composition among studies, in this study, the proportion of Bacteroidetes in the OLP group was higher than in the HC group (
Figure 2A). This finding is in line with the results of Choi et al. [
32], in which there was an increase in Bacteroides in patients with OLP compared to HC [
32]. Bacteroidetes is a gram-negative bacteria considered a significant clinical pathogen, commonly observed in anaerobic infections. Bacteroidetes can induce anti-inflammatory T cell lymphocytes with their antigens in the intestinal tract. Additionally, they have been found to be abundant in conditions such as endocarditis, meningitis, septic arthritis, and osteomyelitis [
33,
34].
At the genus level, the proportion of
Prevotella was higher compared to HC (
Figure 2B). In general, the most abundant bacterium in HC is
Streptococcus, but in the OLP group, the proportion of
Streptococcus decreased and
Prevotella was the most abundant [
32].
Prevotella spp. are anaerobic gram-negative bacteria belonging to the Bacteroidetes phylum. They are commonly found as commensal colonizers at mucosal sites, as well as in saliva and several oral sites.
Prevotella strains are generally considered commensal bacteria due to their extensive presence in the healthy human body and their rare involvement in infections. However, recent studies have linked an increased abundance of
Prevotella and specific strains to inflammatory disorders. This suggests that some strains may exhibit pathobiontic properties. It is important to note that these findings are still emerging and require further investigation. Recent research has shown that the presence of
Prevotella in biofilms of gingivitis and periodontitis can cause periodontitis, similar to
P. gingivalis, which has traditionally been the focus [
35]. In vitro studies have demonstrated that
Prevotella has a greater ability to induce proinflammatory cytokines such as IL-6, IL-8, and tumor necrosis factor-α (TNF-α) compared to strict commensal oral bacteria and even
P. gingivalis [
36]. Components of bacterial cells activate Toll-like receptors (TLRs), with TLR4 primarily recognizing gram-negative bacteria [
37]. Stimulation of TLR4 can lead to the production of proinflammatory cytokines, anti-inflammatory cytokines, and chemokines, as well as the initiation of inflammatory processes. Additionally, TLR signaling by
Prevotella spp. can activate alternative NF-kB signaling [
38].
In Salem et al.’s [
39] study, the transcription of TLR4 was found to be upregulated in the oral epithelium of patients with OLP when compared to HC. This led to the reinforcement of TLR4 reactivity by the recruitment of T lymphocytes, resulting in a proinflammatory loop cycle. Additionally, OLP patients had higher concentrations of NF-κB-dependent cytokines TNF-α, IL-1α, IL-6, and IL-8 compared to HC [
40,
41,
42]. Previous studies indicate that
Prevotella may act as an antigen for T cell-mediated inflammation in OLP.
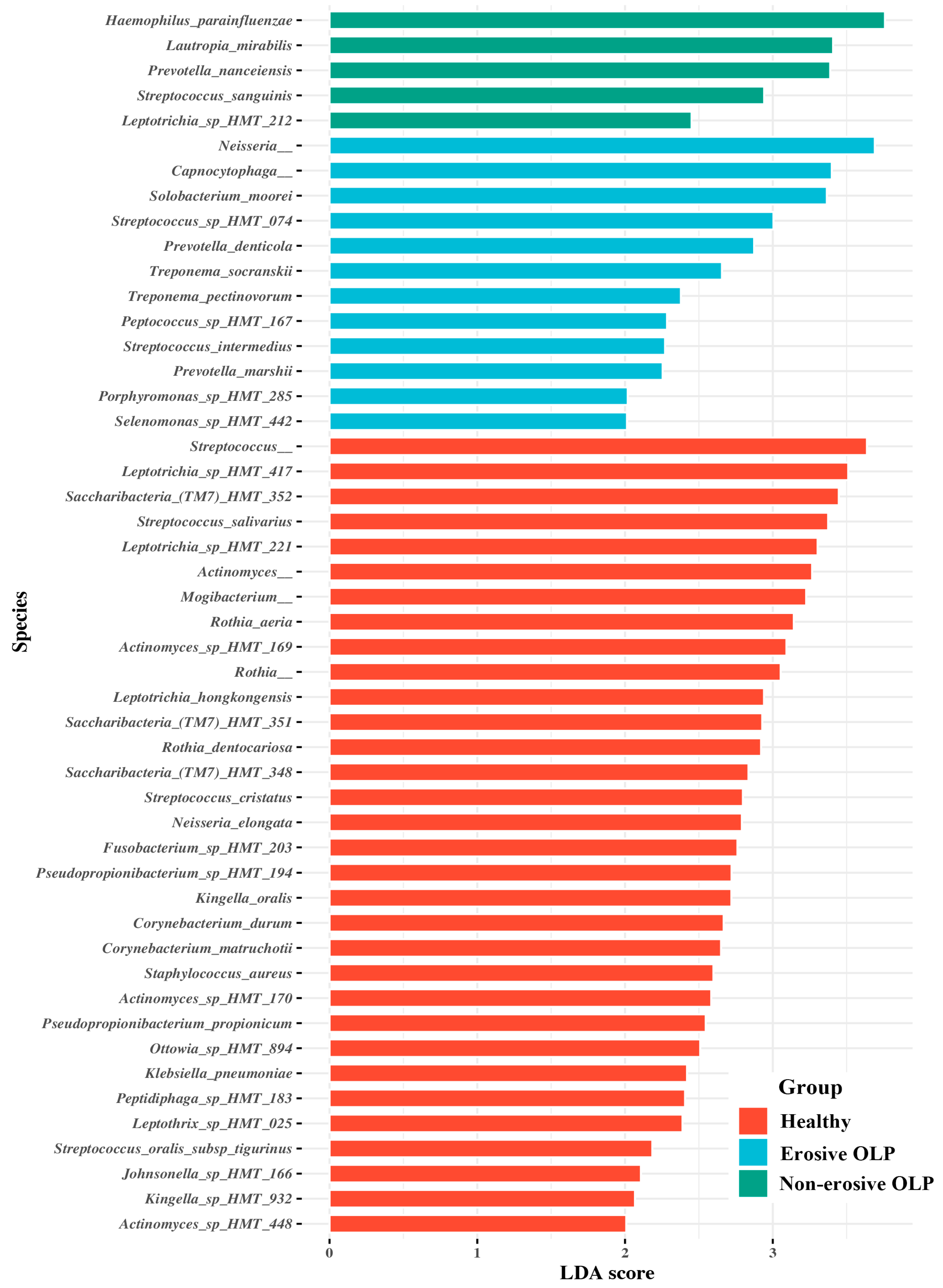
In the E-OLP group,
Prevotella denticola and
Treponema socranskii, which are also frequently observed in patients with chronic periodontitis [
43], were among the significant taxa. Several studies have reported a correlation between OLP and periodontitis. Periodontitis is an inflammatory disease mediated by the host, which begins with the formation of bacterial biofilm and leads to gingival inflammation. OLP is also an inflammatory disease caused by an unknown antigen and is often painful, particularly in the case of E-OLP, which makes oral hygiene challenging. This difficulty leads to the accumulation of plaque and calculus, increasing the risk of long-term periodontal disease [
44]. Conversely, the presence of these plaques and calculus can act as antigens and exacerbate OLP, and adequate plaque control has been shown to improve symptoms in patients with OLP with gingival involvement [
45,
46,
47]. The relative proportions of
Treponema spp. and
Porphyromonas spp. were also higher in this study. This suggests that bacteria associated with periodontitis may also contribute to the inflammatory response in OLP (
Figure 3).
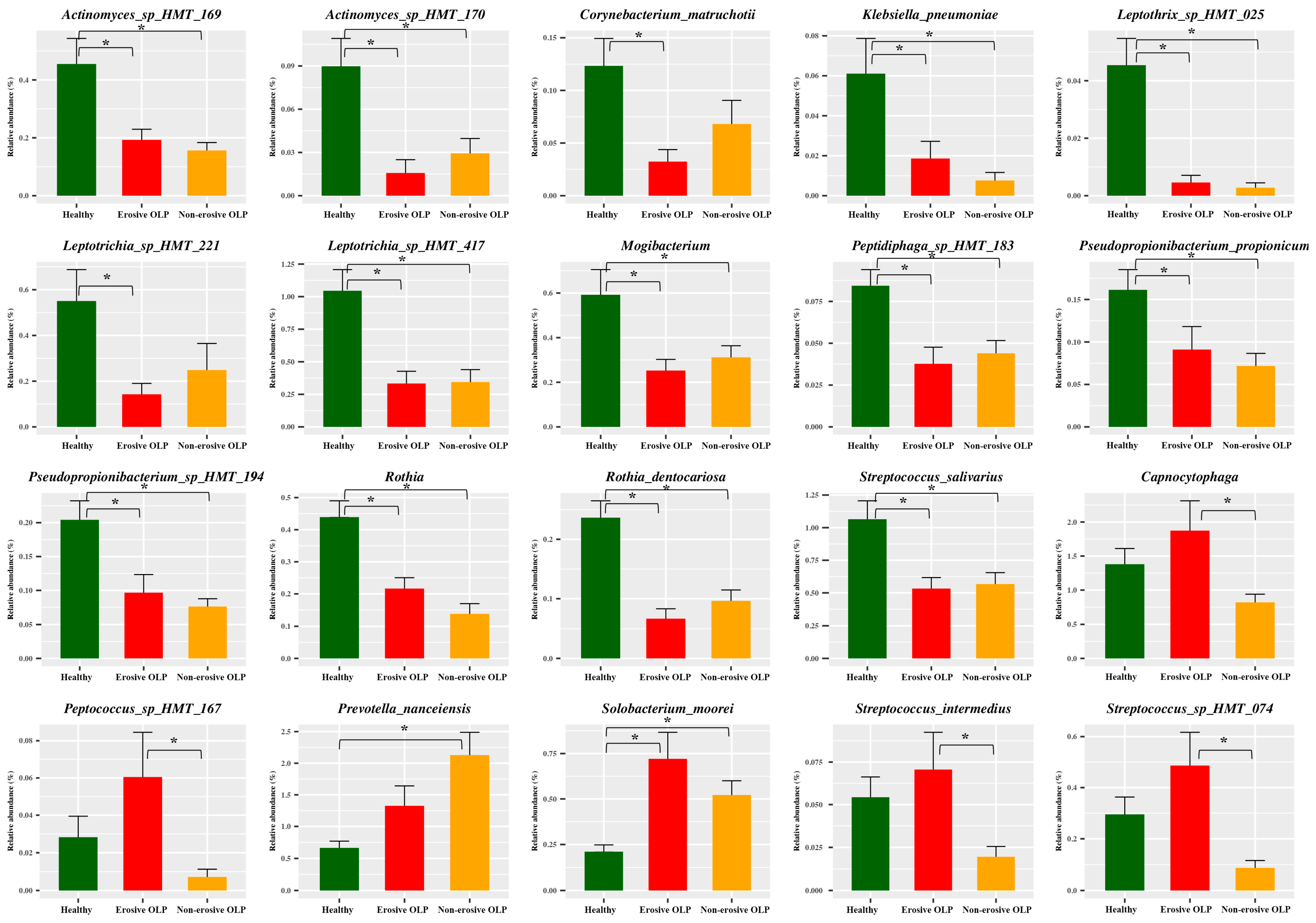
Interestingly,
Capnocytophga and
Peptococcus were relatively more abundant in E-OLP but less abundant in NE-OLP compared to healthy subjects (
Figure 4).
Capnocytophga and
Peptococcus are commonly observed in patients with gingivitis and halitosis, suggesting that NE-OLP may be less difficult to control than E-OLP and may be as well controlled in healthy individuals [
48,
49]. Thus, it may also be important to differentiate between E-OLP and NE-OLP when investigating, planning treatment, and managing patients with OLP.
This study has several limitations. Although the sample size is larger than in previous studies (with an average of 20 patients per group), a larger study is needed to account for other subject-related factors. Secondly, this study did not evaluate the periodontal status of OLP patients, and it was not possible to completely distinguish the periodontal disease from OLP. However, OLP patients before treatment are almost always accompanied by periodontitis due to pain, making it challenging to separate the two conditions. Thirdly, the direct causal role of these bacteria in the development and exacerbation of OLP has not been established. Nevertheless, we believe this study is valuable, as it contributes to the growing body of research at the intersection of OLP and microbiome studies, which have yet to yield consistent results due to variations in research methods.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}