We successfully included oxygen sensitive MRI with an oxygen breathing challenge as part of a multi-parametric MRI assessment of 10 men with biopsy-proven prostate cancer as part of the planning for surgical resection.
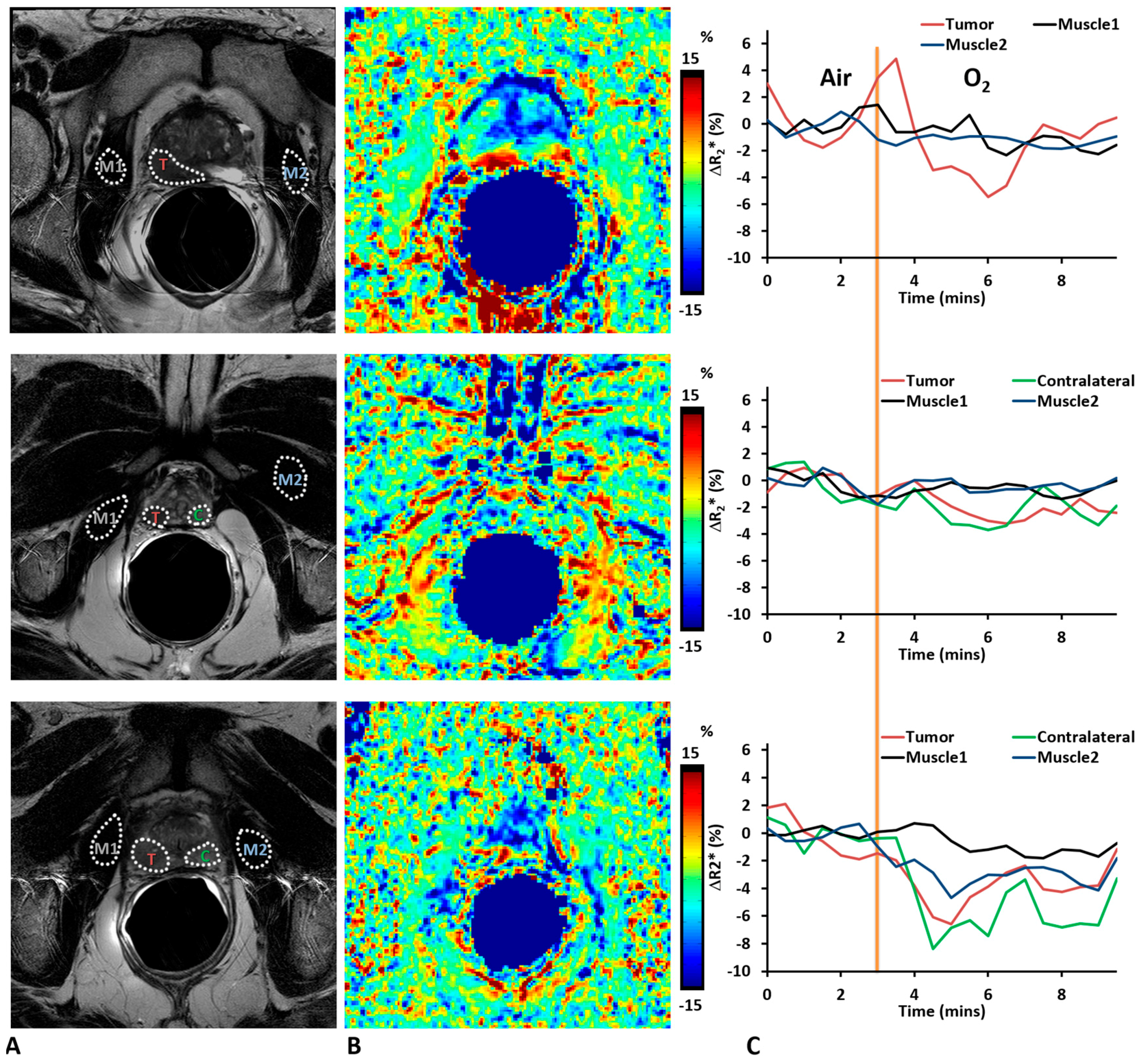
In this study, we included BOLD and TOLD studies with oxygen challenge to assess the tumor response. While there were dynamic variations in R
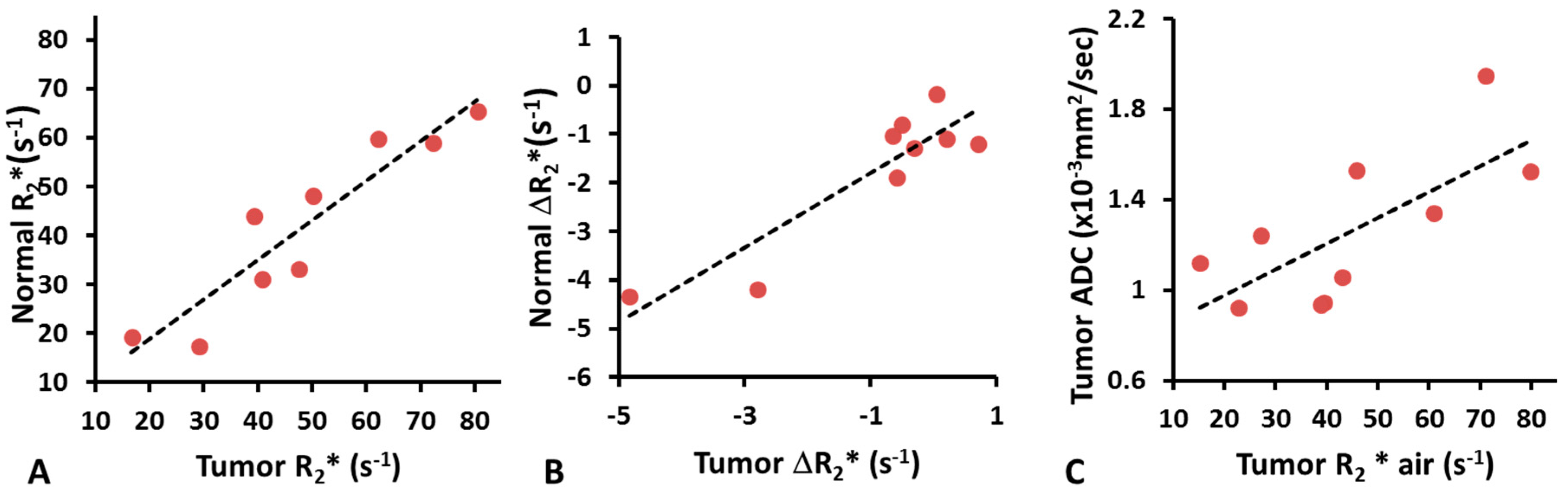
2* for some tumor and normal prostate tissue (
Figure 1), the muscle values were quite stable during both baseline air breathing and in response to oxygen challenge. As to the average ROI measurements of individual patients, both tumor and normal prostate tissue showed a wide range of R
2* values indicating significant individual variation, while R
2* of reference muscle was similar among patients ensuring the variation was not scan protocol related. We found baseline tumor R
2* was significantly higher than that of normal prostate. Significantly greater change in R
2* was found upon oxygen breathing in tumor compared with normal prostate. No correlation was found between ΔR
2* and Gleason score. However, ΔR
2* showed a trend with AUC and MIP (
R2 > 0.3). We also noticed that R
2* (air and 100% oxygen) showed correlation with Gleason score. Chopra et al. [
12] showed a correlation between R
2* and hypoxic fraction < 5 Torr (HF
5) assessed by an Eppendorf needle electrode, but did not attempt an oxygen breathing challenge. Alonzi et al. [
14] used a carbogen breathing challenge (so-called carbogen lite with 2% CO
2 to mitigate patient stress) and reported a reduction in R
2* in tumors for nine of 14 patients with a mean reduction in R
2* of 3.52 s
−1 or 21.6% (
p = 0.0005) at 1.5 T. We observed a mean reduction ΔR
2* = 1.64 s
−1 for the 10 tumors, which was significant for the group based on paired
t-test (
p < 0.01). Diergarten et al. [
16] used a conventional carbogen challenge (5% CO
2) to examine 29 patients with biopsy proven cancer followed by radical prostatectomy and reported BOLD response to be lower than normal contralateral prostate at 1.5 T. These previous studies did not attempt to correlate BOLD response with Gleason score or other MRI parameters. The ability to induce changes in tumor R
2* using oxygen rather than carbogen breathing suggests easier implementation into human studies, since carbogen is recognized as frequently causing respiratory distress. However, highly variable response was observed, which was transient in many cases. Such behavior has also been reported in pre-clinical studies of human PC3 xenografts in mice and large Dunning prostate R3327-AT1 tumors in rats [
14,
18]. Given the small ΔR
2*, it is not surprising that ΔR
1 was not significant, since the TOLD response is generally reported to be much smaller than BOLD [
18]. The small changes are commensurate with hypoxic tumors, which are not readily amenable to modulation [
24], though this has not been confirmed here. BOLD MRI with an oxygen breathing challenge has previously been applied to patients with cancer of the cervix at 3 T [
41]. The R
2* values tended to be somewhat smaller in cervical tumors (mean 23.5 s
−1) with a mean response of −1.1%, as compared with −3.6% here. It has also been reported that R
1 of lipids may provide enhanced sensitivity to changes in pO
2 using the so-called MOBILE approach [
42], although a subsequent study at higher field found R
1 of the water signal to be more sensitive [
25]. MRI-based oxygen imaging (MOXI) [
43] has been reported to provide quantitative tumor oxygenation measurements in preclinical settings and it will be interesting to apply such techniques to cancer patients in due course.
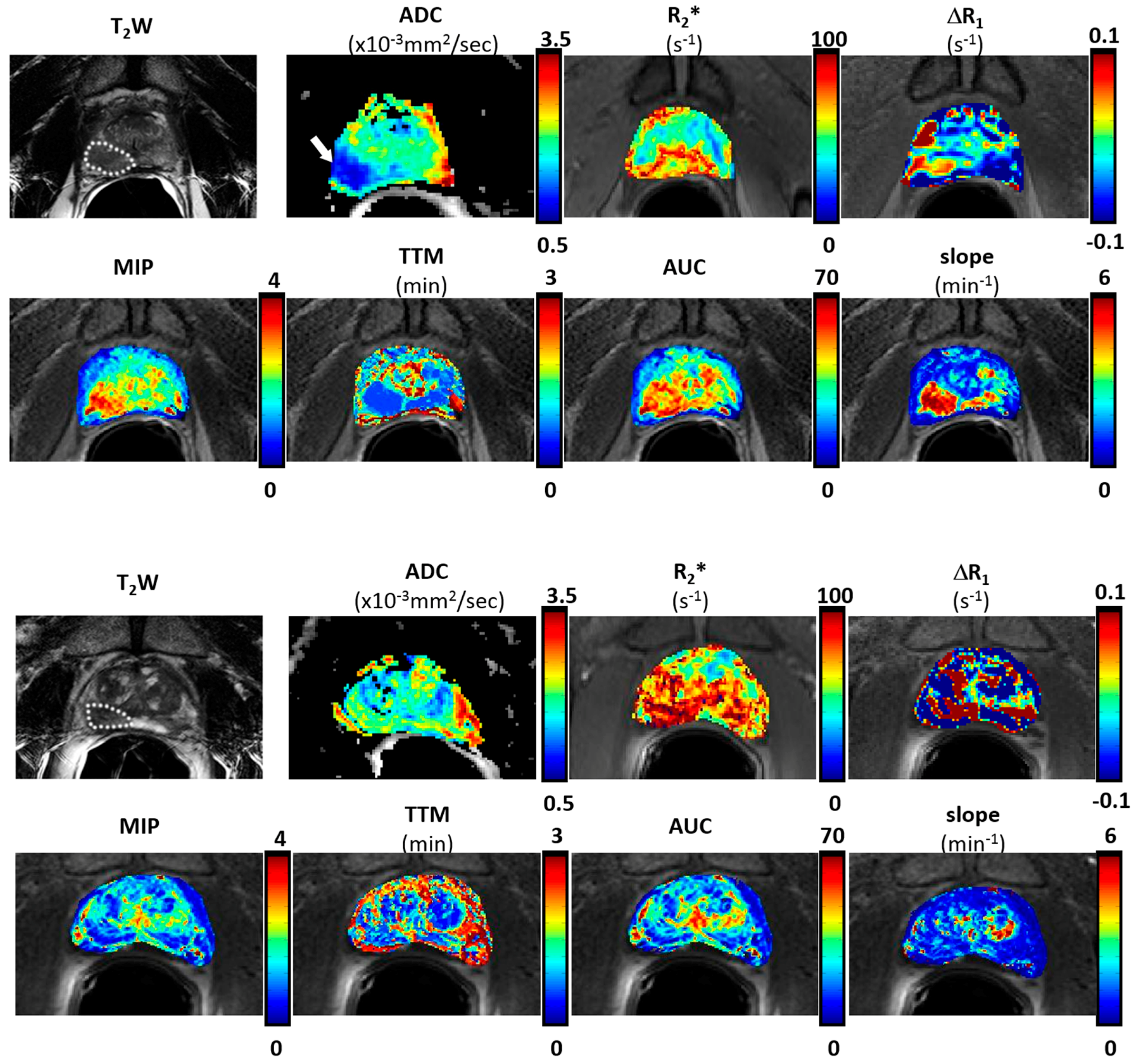
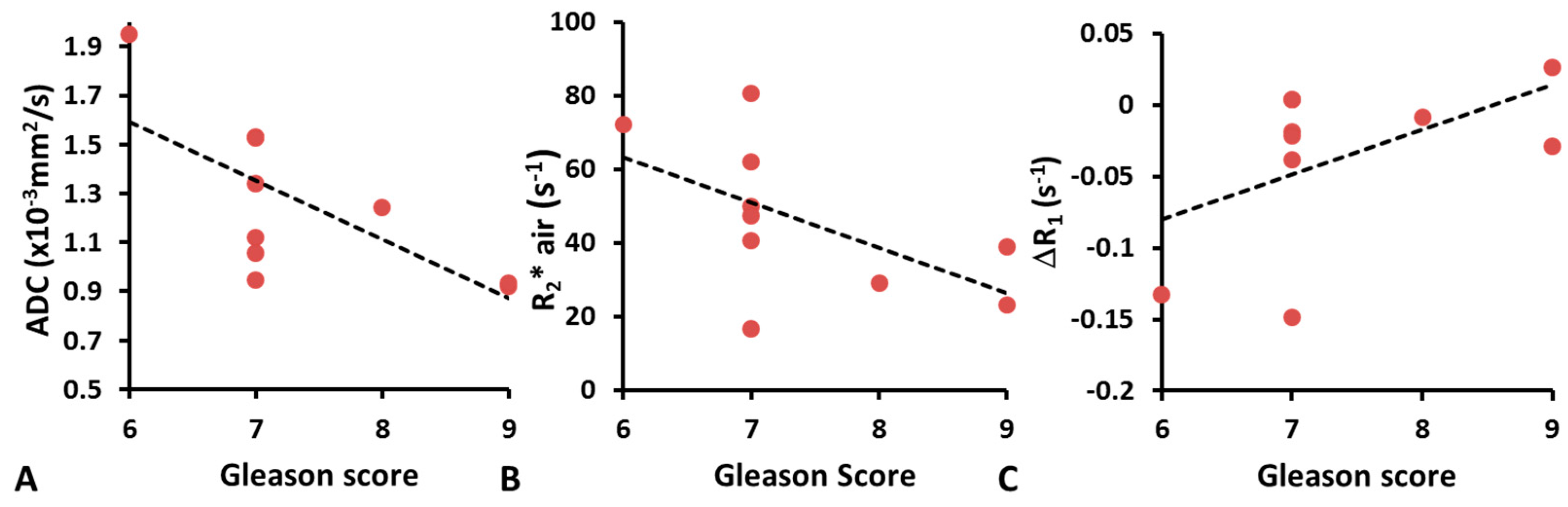
Diffusion weighted MR imaging is a noninvasive technique that explores the Brownian motion of water in tissue. Recent studies showed that ADC was useful in detecting high grade lesions that might be missed by standard biopsies [
37]. We found moderate correlation between ADC and Gleason score (
R2 = 0.48;
p < 0.05) in line with previous reports [
7,
37,
38,
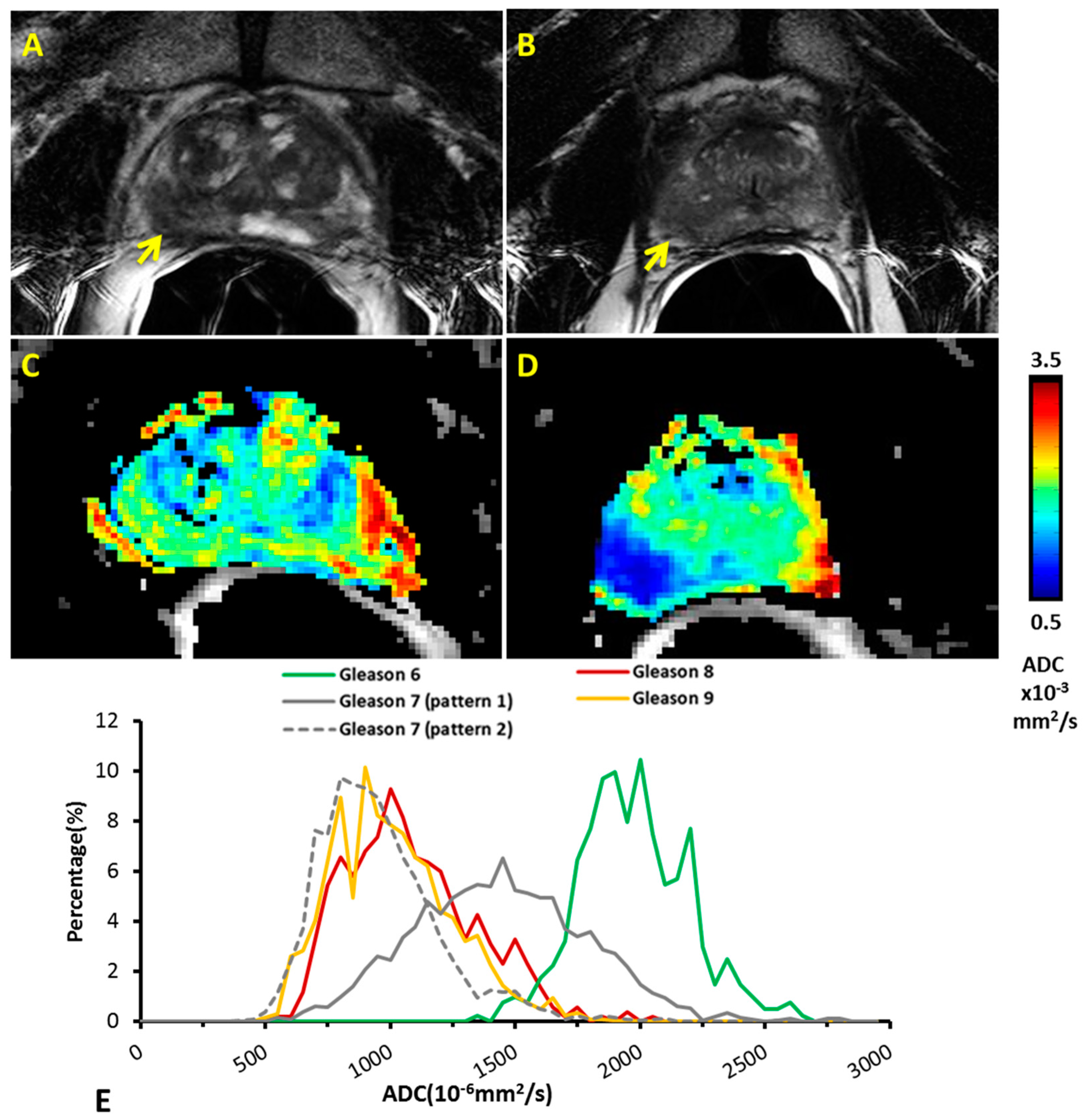
44]. The different ADC between high and low grade prostate tumor likely reflects the increase in cellularity as tumors progress [
45]. We noticed that patients with Gleason score 7 had two distinct histogram patterns. Three patients showed ADC distribution similar to high grade classification. A wide range of ADC values for Gleason score 7 have been reported previously, potentially associated with a wide range of cellularity and biological behaviors for intermediate Gleason score 7 [
40,
46,
47,
48]. Since our patients underwent prostatectomy soon after MRI, we were not able to relate any of the MRI results with tumor progression. This could be explored in patients undergoing radiation and/or chemotherapy.
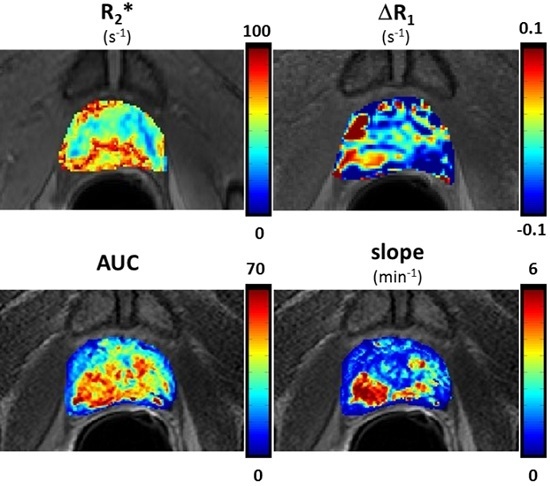
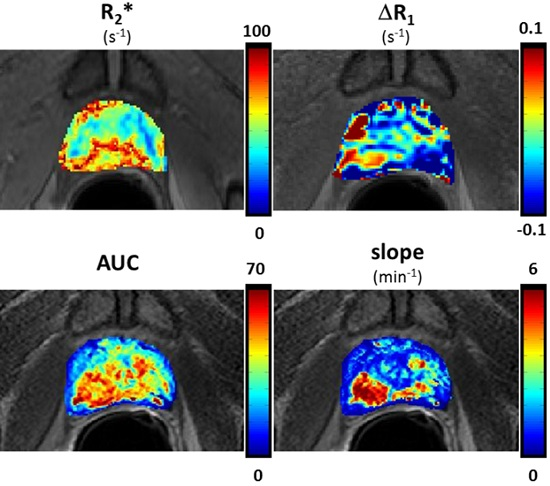
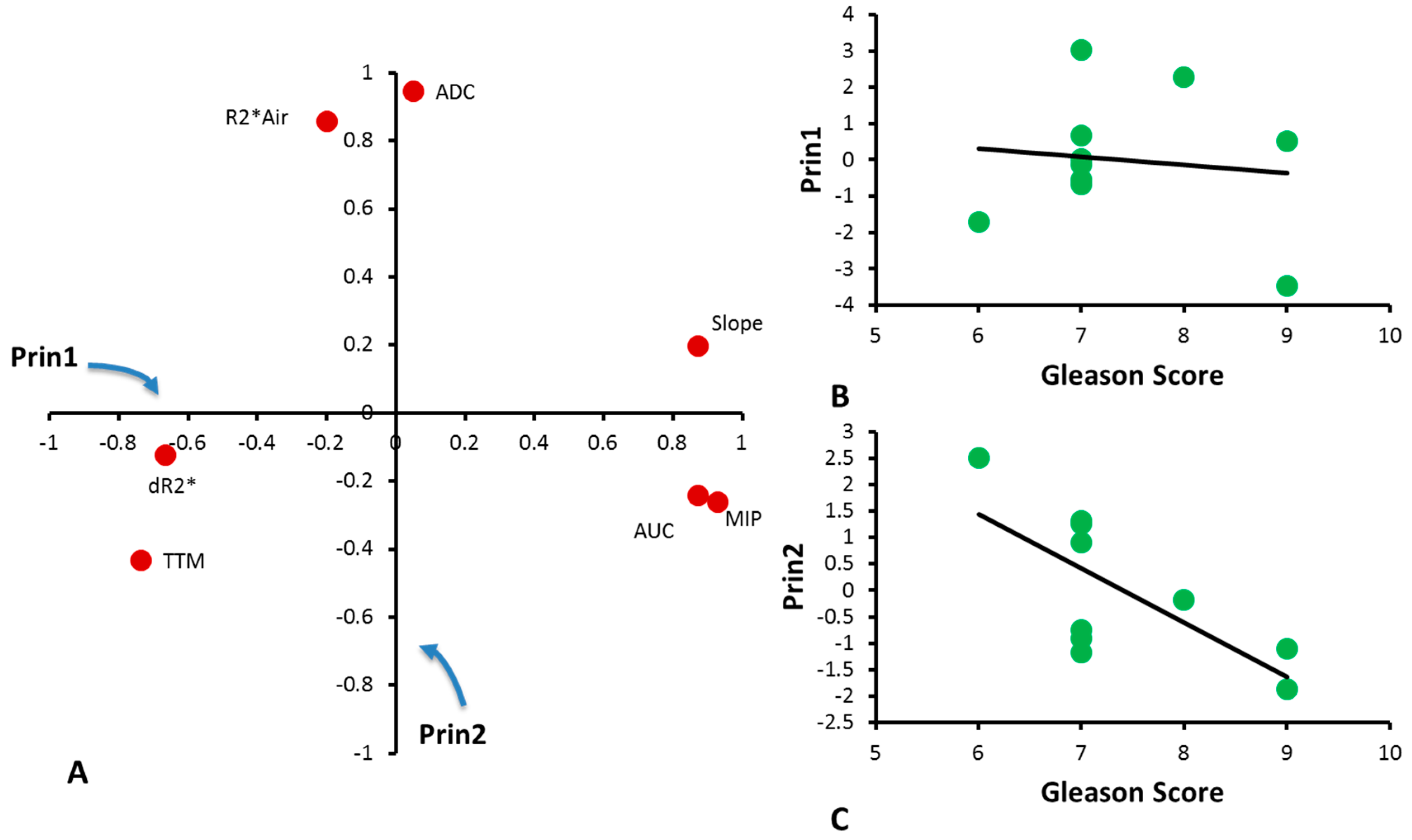
Principal Component Analysis is a statistical technique widely used for data reduction. It has previously been used in DCE analysis of CaP to recognize different enhancement patterns without the need for kinetic modeling [
49]. Principal Component Analysis does not appear to have been applied to multi-parametric MRI previously. The main Principal Components identified by Principal Component Analysis represent the blood perfusion-related variables (Prin1, which is mainly attributed to ΔR
2*, MIP, TTM, slope and AUC) and tissue composition and cellularity-related variables (Prin2, which is mainly attributed to baseline R
2* and ADC). Correlation of the Gleason score with Prin2, but not Prin1, is reasonable, considering that the Gleason score is based on the cellular composition of the specimens. Further investigation of Principal Component Analysis with respect to histology could enhance the understanding of the Principal Components, and results will need to be validated in a larger study. We examined feasibility of data reduction based on Principal Component Analysis, but another approach is to evaluate multiparametric characteristics of tumor regions, based on cluster analysis or using one parameter to identify regions of response and apply a mask to a second parameter. Recent work reported that DCE could be used to identify well-perfused areas from hypoxic regions, and assist in correlating TOLD response with histological assessments in some tumors [
50].
This study presents preliminary results of BOLD and TOLD responses to oxygen breathing in a small cohort of CaP patients. The number of patients and especially number of patients with low and high Gleason score was small, limiting the strength of the conclusions. A larger study should allow further risk stratification, including criteria such as tumor bulk, and PSA values and dynamics, as per the National Comprehensive Cancer Network (NCCN) guidelines. Correlation with the MRI-derived Prostate Imaging Reporting and Data System (PI-RADS) scores [
4,
51] and the Prostate Diagnostic Imaging Consensus Meeting panel proposed five-point Likert scaling [
2,
3] will also be pertinent, but the goal here was proof of principle to demonstrate the feasibility of including oxygen-enhanced MRI. In particular, a TOLD response has not been reported in human CaP patients previously. Rigorous immunohistological correlates could also be valuable, and the recent development of 3D printed customized molds will ensure better registration of imaging and histology. Another limitation was the use of only three
b-values (0, 500 and 1000), due to time constraints. This limited the accuracy of ADC calculation and prevented further analysis with more sophisticated algorithms, such as the Intravoxel Incoherent Motion (IVIM) modeling.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}