1. Introduction
Infections caused by third-generation cephalosporin-resistant
Enterobacteriaceae mediated mainly by the expression of extended-spectrum β-lactamases (ESBL) have increased significantly, thereby posing great challenges to clinicians by restricting the choice of antimicrobial agents [
1,
2]. Data from a report by the European Antimicrobial Resistance Surveillance Network in 2019 indicated that 15.1% of
Escherichia coli and 31.7% of
Klebsiella pneumoniae were resistant to third-generation cephalosporins [
3], while the rate was reported to be as high as 61.3% for
E. coli and 60.3% for
K. pneumoniae in a Chinese study from 2018 [
4]. The clinical impact of ESBL-producing
Enterobacteriaceae has been well studied, as these pathogens cause worse clinical outcomes when compared with their non-ESBL-producing counterparts [
5]. A recent meta-analysis including 84 studies with 22,030 patients reported increased attributable mortality by a factor of 1.75 (95% CI, 1.45–2.11) in bloodstream infections caused by ESBL-producing
Enterobacteriaceae [
6].
Carbapenems are typically the first-choice antibiotics recommended by clinical guidelines to treat infections caused by ESBL-producing
Enterobacteriaceae [
7,
8]. They withstand hydrolysis by ESBL enzymes well and therefore present good activity against these pathogens [
9,
10,
11]. A recent study that collected 7168 clinical isolates of
Enterobacteriaceae from patients in the USA and Europe between 2016 and 2018 demonstrated a high susceptibility rate to meropenem at 97.6% in isolates with the ESBL genotype [
12]. Similarly good in vitro activity was also described in a Chinese study, with the susceptibility rate to imipenem of ESBL-producing
E. coli being 99.7% and that of ESBL-producing
K. pneumoniae being 98% [
13]. However, the increased use of carbapenems has led to the emergence of carbapenem-resistant bacteria, which places an added burden on public health [
14,
15]. Therefore, it is urgently necessary to find an effective carbapenem-sparing therapy for infections caused by ESBL-producing
Enterobacteriaceae.
Classic β-lactam/β-lactamase inhibitor combinations, such as amoxicillin/clavulanate, ampicillin/sulbactam, cefoperazone/sulbactam, and piperacillin/tazobactam, usually demonstrate good in vitro activity against ESBL-producing
Enterobacteriaceae when these pathogens do not possess other antimicrobial resistant mechanism(s) [
10,
12]. Among the available classic β-lactam/β-lactamase inhibitor combinations, piperacillin/tazobactam is one of the most interesting carbapenem-sparing therapies against infections caused by ESBL-producing
Enterobacteriaceae [
9,
16]. A recent antimicrobial resistance surveillance study indicated that the susceptibility of
Enterobacteriaceae with the ESBL genotype to piperacillin/tazobactam was as high as 71.4%, compared to only 18% and 11.9% for amoxicillin/clavulanate and amoxicillin/sulbactam, respectively [
12]. Clinical studies have demonstrated the comparable effectiveness of piperacillin/tazobactam and carbapenems in the treatment of urinary tract infections [
17,
18,
19]. However, the efficacy of piperacillin/tazobactam in treating bacteremia caused by ESBL-producing
Enterobacteriaceae is still uncertain, as some studies have indicated comparable effectiveness [
20,
21,
22,
23,
24] while some have demonstrated inferiority [
25,
26,
27].
Evidence supporting the use of β-lactam/β-lactamase inhibitor combinations in the treatment of bloodstream infections due to ESBL-producers is primarily based on the INCREMENT study, a multinational, preregistered cohort study with a large sample size, in which the 30-day mortality did not show any statistical differences between β-lactam/β-lactamase inhibitor combinations (amoxicillin/clavulanate and piperacillin/tazobactam) and carbapenems (ertapenem, meropenem, imipenem, and doripenem) in both empiric and definitive therapy cohorts [
20]. Moreover, there were no differences detected between amoxicillin/clavulanate and piperacillin/tazobactam versus carbapenems in the subgroup analysis, indicating support for the use of the β-lactam/β-lactamase inhibitor combination to minimize carbapenem use [
20]. Similar results were subsequently published in two meta-analyses [
28,
29].
By contrast, the MERINO trial, which compared piperacillin/tazobactam with meropenem in the treatment of bloodstream infections caused by ceftriaxone-resistant
E. coli or
K. pneumoniae did not support the use of piperacillin/tazobactam [
27]. The 30-day mortality in patients receiving piperacillin/tazobactam was statistically higher than that of those receiving meropenem (12.3% vs. 3.7%) [
27]. However, a post hoc analysis by the same group of authors, which involved re-performing the antimicrobial susceptibility testing with the referred broth microdilution methods, did not support the inferiority of piperacillin/tazobactam [
21]. It found that there were a significant proportion of piperacillin/tazobactam non-susceptible strains included in the MERINO trial, and when those non-susceptible strains were excluded the between group difference in 30-day mortality was reduced to 5% (95% CI, −1% to 10%) [
21]. Therefore, it can be concluded that piperacillin/tazobactam is as effective as meropenem in treating bacteremia caused by piperacillin/tazobactam-susceptible ESBL-producers.
Because there have not been any clinical studies dedicated to the therapeutic options for pneumonia caused by ESBL-producing
Enterobacteriaceae, guidelines [
7,
8] against using piperacillin/tazobactam in such cases has been largely based on the original findings by Harris et al. [
27] in the MERINO trial. However, when considering the aforementioned factors of the MERINO trial described two years later by Henderson et al. [
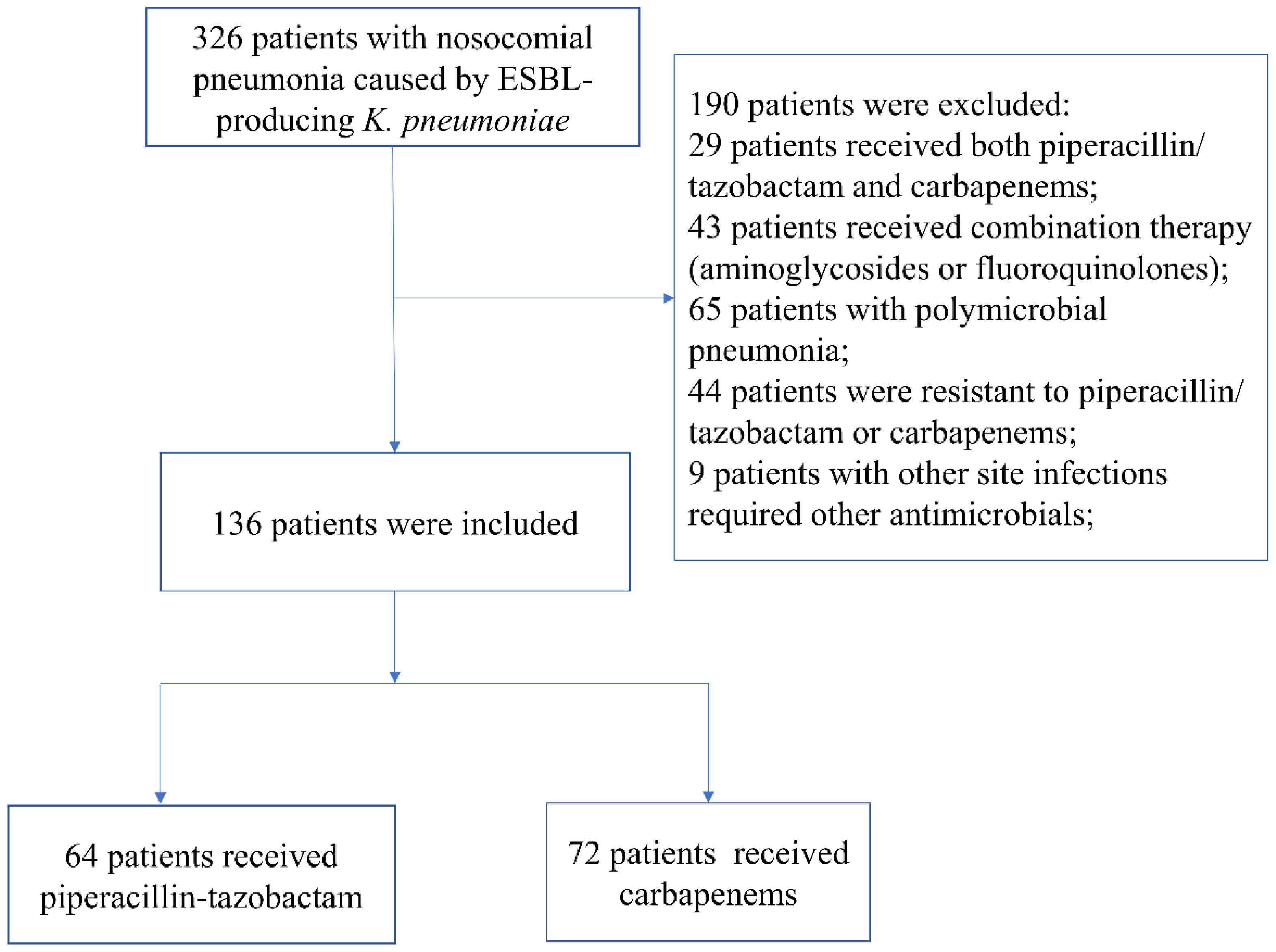
21], it is reasonable to hypothesize that piperacillin/tazobactam might be an effective alternative to carbapenems for treating pneumonia caused by ESBL-producers if susceptibility is established. Therefore, we conducted this retrospective cohort study to test this hypothesis by treating patients with nosocomial pneumonia caused by ESBL-producing
K. pneumoniae with either carbapenems or piperacillin/tazobactam.
4. Discussion
Although many studies have assessed the effectiveness of piperacillin/tazobactam at treating various infections caused by ESBL-producing
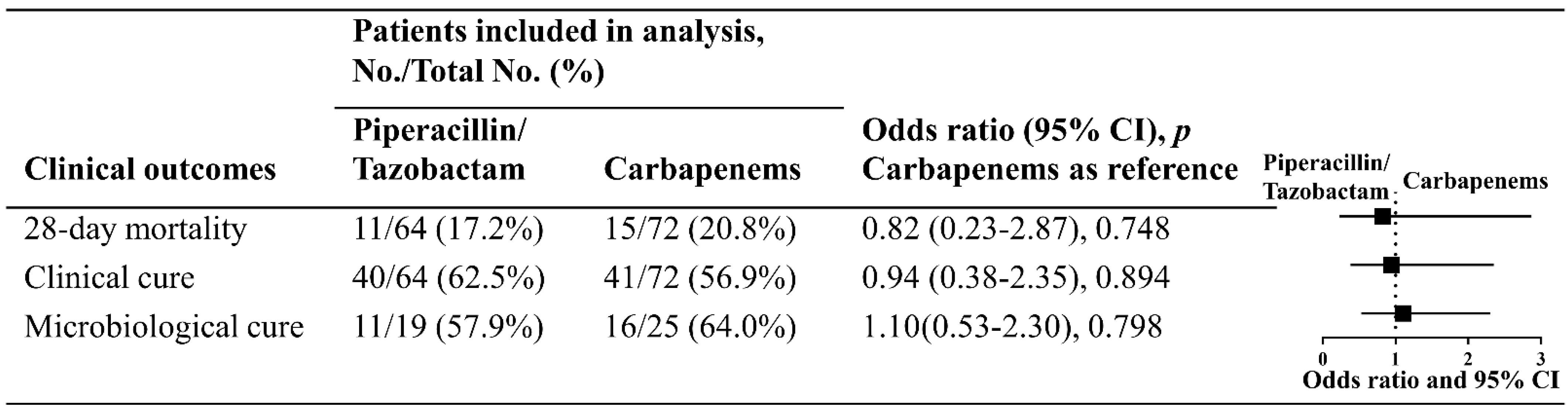
Enterobacteriaceae, there have not been any published studies specifically evaluating its efficacy at treating pneumonia caused by these pathogens. In the present study, we assessed the effectiveness of piperacillin/tazobactam at treating patients with nosocomial pneumonia due to ESBL-producing
K. pneumoniae in comparison with carbapenems. The results suggest that piperacillin/tazobactam might be an effective alternative to carbapenems in treating such infections, as it resulted in similar 28-day mortality and 14-day clinical and microbiological cure. Clearly, our results differ from some studies that came to negative conclusions regarding the effectiveness of piperacillin/tazobactam in the treatment of bacteremia due to ESBL-producing
Enterobacteriaceae (or ceftriaxone-resistant bacteria), which has been summarized and discussed in reviews [
38,
39,
40,
41,
42]. Next, two important factors that might contribute to the different outcomes of such studies, i.e., the MIC breakpoints of piperacillin/tazobactam and the dosing/administration model used, will be discussed.
Which breakpoint of MIC for piperacillin/tazobactam is used to interpret the results of antimicrobial susceptibility testing against ESBL-producers matters greatly. The susceptible breakpoint of piperacillin/tazobactam in EUCAST is ≤8 mg/L, while it is ≤16 mg/L in CLSI [
31,
33]. Accordingly, ESBL-producers with an MIC between 8 and 16 mg/L have been included in studies using the CLSI breakpoint while they have been excluded in studies using the EUCAST breakpoint. The inclusion of patients with technical uncertainty (8 to 16 mg/L) who were subsequently treated with piperacillin/tazobactam would have probably affected clinical outcomes. A pharmacokinetic and pharmacodynamic (PK/PD) study indicated that the success rate of piperacillin/tazobactam (4 g every 6 h) achieving the target against ESBL-producers was 99% when the MIC of ESBL-producers was ≤8 mg/L, while the success rate decreased to 57% when the MIC reached 16 mg/L [
43]. Clinical studies also suggest that the MIC to piperacillin/tazobactam in ESBL-producers was negatively associated with clinical outcomes. In a retrospective study that included patients with bacteremia due to ESBL-producing
E. coli, the mortality rate was 4.5% in patients infected with strains that had an MIC to piperacillin/tazobactam ≤4.5 mg/L, while mortality was significantly increased to 23% in those infected by strains with an MIC ≥ 8 mg/L [
44]. The post hoc analysis of the MERINO trial demonstrated a similar trend [
21]. In patients with bacteremia caused by ceftriaxone-resistant
E. coli or
K. pneumoniae that did not originate from urinary tract infections, the mortality rate in patients receiving piperacillin/tazobactam was 27.3% when the MIC was ≤8 mg/L but increased to 71.4% when the MIC exceeded 8 mg/L [
21]. Moreover, a retrospective study including patients with bacteremia caused by cefotaxime non-susceptible
E. coli and
K. pneumonia with a MIC to piperacillin/tazobactam ≤ 8 mg/L (70.7% patients infected by strains with an MIC of ≤4 mg/L, 29.3% patients by strains with an MIC of ≤8 mg/L) indicated comparable outcomes between piperacillin/tazobactam and carbapenems [
45]. By contrast, another study comprising patients with bacteremia due to ESBL-producing bacteria with a higher MIC distribution (all ≤16 mg/L, 39% ≤4 mg/L, 46% ≤8 mg/L, and 14% ≤16 mg/L) demonstrated a worse clinical outcome in patients empirically receiving piperacillin/tazobactam [
25]. Together with the results found in our study, where the EUCAST cut-off was used, it is reasonable to recommend restricting piperacillin/tazobactam use to ESBL-producers with an MIC of ≤8 mg/L.
A second factor that affects clinical outcomes is the dosing and administration model of piperacillin/tazobactam. Since piperacillin/tazobactam is a time-dependent antibiotic combination, the antimicrobial activity depends on the percentage of the dosing interval that the free drug concentration is maintained above the MIC of the target pathogen (
fTMIC) [
46]. PK/PD studies indicated that, compared with intermittent administration of 4 g of piperacillin/tazobactam every 8
h, those using 4.5 g of piperacillin/tazobactam every 6 h or by continuous infusion had higher success rates for achieving the probability of attainment for 50% and 100%
fTMIC [
47,
48]. A systematic review and meta-analysis comparing the prolonged infusion of piperacillin/tazobactam with intermittent infusion in severely ill patients indicated that the prolonged infusion was associated with 1.46-times lower odds of mortality (95% CI, 1.20–1.77) [
49]. Moreover, a retrospective study including patients with bacteremia due to ESBL-producers receiving different doses of piperacillin/tazobactam illustrated the opposite result [
25]. In the subgroup analysis, patients receiving 4.5 g of piperacillin/tazobactam every 6 h did not show any difference in mortality compared with those receiving carbapenems; in contrast, the adjusted death rate was 1.92 times higher for patients receiving piperacillin/tazobactam when compared with those using carbapenems in the whole population, as 61% of patients were receiving 3.375 g of piperacillin/tazobactam every 6 h [
25]. Therefore, the dose and administration model of piperacillin/tazobactam is essential to maintain favorable outcomes. Although the post hoc analysis of the MERINO study supports that intermittent infusion of piperacillin/tazobactam every 6 h was as effective as carbapenems when the pathogens were truly susceptible to it [
21], considering the inoculum effect in the lung [
50], we still recommend using piperacillin/tazobactam 4.5 g every 6 h by extended infusion (3 to 4 h) or continuous infusion for pneumonia, as was carried out in our study.
Despite the promising results of piperacillin/tazobactam demonstrated in this study, using this combination to treat ESBL-producing infections still needs to be assessed with great caution. The inaccuracy in piperacillin/tazobactam susceptibility determined by automatic systems in clinical practice is the primary concern [
51], as was demonstrated by the post hoc analysis of the MERINO trial [
21]. A considerable proportion of isolates were in fact not susceptible to piperacillin/tazobactam by broth microdilution but were categorized as piperacillin/tazobactam susceptible using automatic methods, which subsequently led to the failure of piperacillin/tazobactam therapy [
21,
27]. The inaccurate susceptibility of piperacillin/tazobactam in these ESBL-producing pathogens was due to the coharboring OXA-1 (oxacillinase-1) [
51]. Studies have illustrated that pathogens coharboring OXA-1 and ESBL may show false susceptibility to piperacillin/tazobactam when measured with the Vitek 2 automatic system [
52] or strip-gradient test (Etest) [
21]. Nevertheless, it is still possible to account for this disadvantage in clinical practice. Isolates coharboring OXA-1 and ESBL that were associated with elevated piperacillin/tazobactam MICs [
21] typically had the MIC of piperacillin/tazobactam at 8 to 16 mg/L [
52], the area of technical uncertainty, a concept introduced by the EUCAST to account for the challenge of test variability [
31]. Therefore, restricting the use of piperacillin/tazobactam to isolates with an MIC < 8 mg/L, the lower breakpoint of piperacillin/tazobactam suggested by EUCAST, makes it less likely to include clinically relevant OXA-1 strains in piperacillin/tazobactam therapy.
Apart from the coharboring OXA-1, the coexistence of AmpCs (Ambler Class C β-lactamases) in ESBL-producing bacteria is another concern when using piperacillin/tazobactam. Studies have reported that a significant proportion of
Enterobacteriaceae coharbor both AmpC and ESBL [
21,
53]. AmpCs typically cause resistance against tazobactam, thereby also diminishing the efficacy of piperacillin in such pathogens [
54]. As AmpCs are not routinely tested in clinical practice, this might add uncertainty to clinical decisions to use piperacillin/tazobactam in ESBL-producing bacterial infections. However, from the perspective of clinicians, it is very unlikely that they would use piperacillin/tazobactam in isolates coharboring both ESBL and clinically relevant AmpCs when the choice of antibiotics was made based on the results of antimicrobial susceptibility testing. Enterobacterales with plasmid-mediated
ampC or derepressed chromosomal
ampC usually express AmpC at a clinically relevant level and cause resistance against piperacillin/tazobactam [
54,
55]; in contrast, strains harboring chromosomal
ampC but still exhibiting susceptibility to piperacillin/tazobactam generally express the AmpC at a very low level and they usually do not cause a clinical issue, similar to the chromosomal
ampC in many
E. coli strains [
54,
56]. Moreover, both piperacillin and tazobactam are weak inducers of AmpC enzymes [
57]. Clinical studies have already demonstrated that piperacillin/tazobactam resulted in similar clinical outcomes to carbapenems when treating infections caused by ESBL-producing pathogens that expressed AmpC but are still susceptible to piperacillin/tazobactam [
58,
59]. Taken together, when considering using piperacillin/tazobactam to treat ESBL-producing infections, the accurate phenotypical susceptibility needs to be determined on top of the genomic background of the clinical isolates.
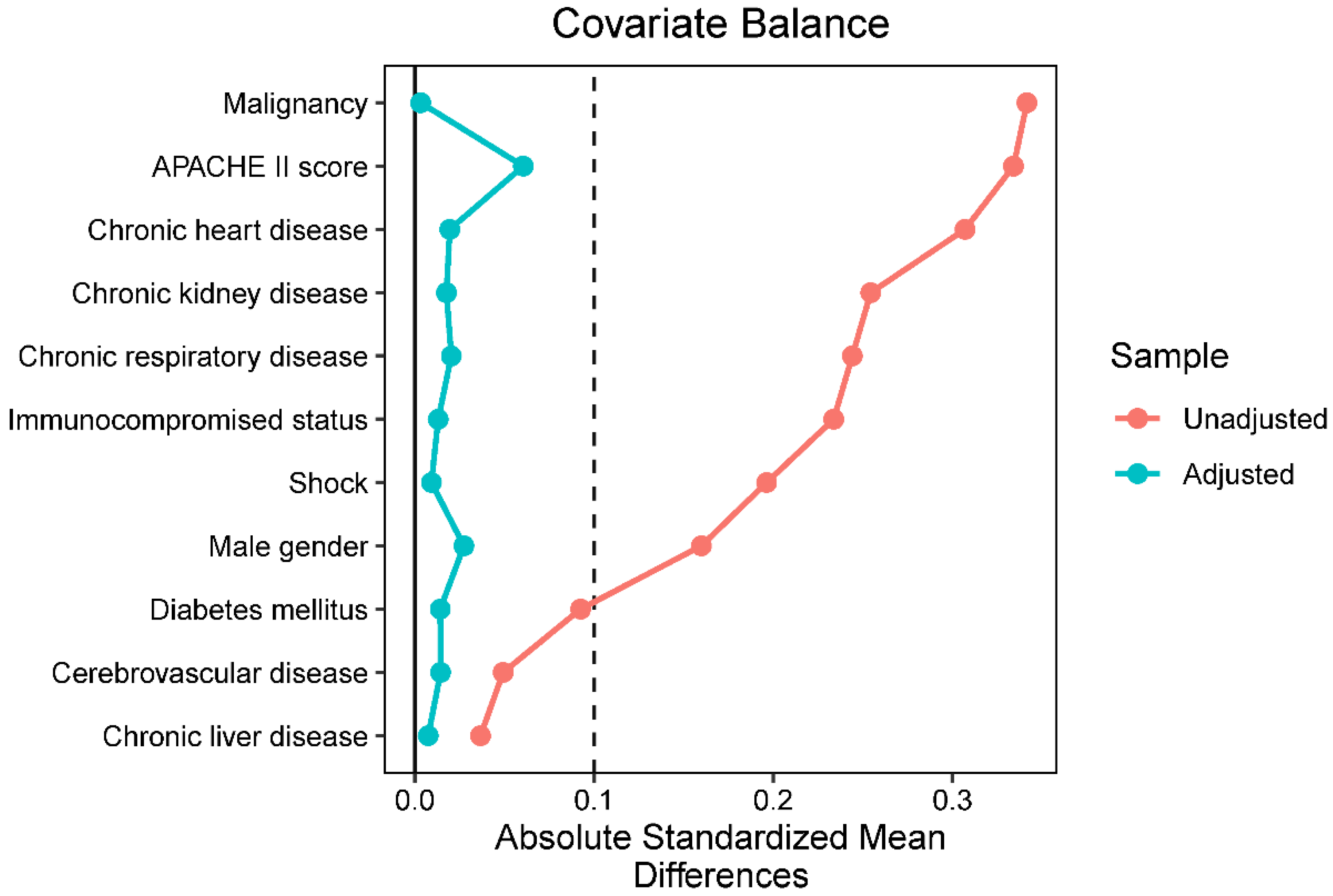
There are several limitations in the present study. First, it has a small sample size and is a retrospective study. Bias and confounders might still affect the final analysis despite implementing the propensity score weighting. Second, ESBL-production was determined phenotypically by the automatic Vitek 2 system instead of by the referred methods [
33]. Although studies have indicated the excellent sensitivity and specificity of the Vitek 2 system [
32,
60], it still might include false-positive isolates in this study, hence skewing the results in favor of piperacillin/tazobactam. Third, the distribution of ESBL enzymes varies geographically [
10,
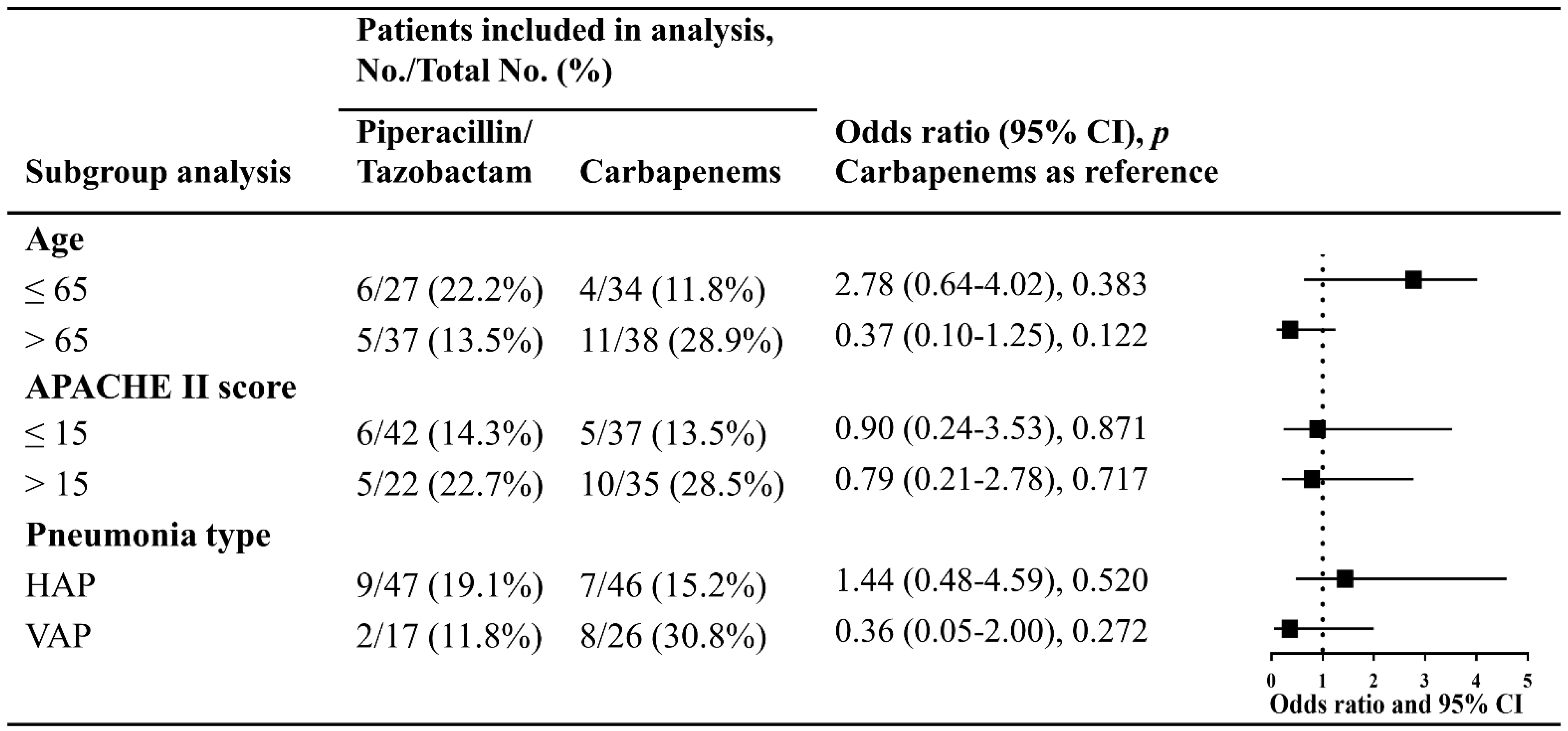
61]; thus, without knowing the genomic background, the results in this study might not be generalizable. Fourth, all patients included in this study displayed mild to moderate pneumonia, and only 11% (15/136) of patients had an APACHE II score >15. Thus, it is unclear how well piperacillin/tazobactam would function in severe patients. Fifth, with a meager rate of blood culture implemented in the study cohort, we did not incorporate the impact of bacteremia in the final analysis. Having this analysis would have strengthened the interpretation of clinical results, as it is known that bacteremia is an independent risk factor for mortality in patients with pneumonia [
62]. Sixth, we only included patients receiving piperacillin/tazobactam or carbapenems starting from the onset of pneumonia; those using piperacillin/tazobactam only for definitive therapy were excluded. Therefore, we were unable to draw any conclusions regarding the efficacy of piperacillin/tazobactam definitive therapy in nosocomial pneumonia due to ESBL-producers. Seventh, in the present study, the economic cost of the two regimens was not incorporated in the final analysis; therefore, which regimen possesses a financial advantage is still unknown. Despite these limitations, to the best of our knowledge, this is the only study to date specifically focused on assessing the clinical effectiveness of piperacillin/tazobactam in the treatment of nosocomial pneumonia due to ESBL-producing
K. pneumonia, and thus this work contributes towards using the most appropriate carbapenem-sparing therapy.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}