
Impact of Systemic Treatments on Outcomes and Quality of Life in Patients with RAS-Positive Stage IV Colorectal Cancer: A Systematic Review

 , and
, and
Abstract
:1. Introduction
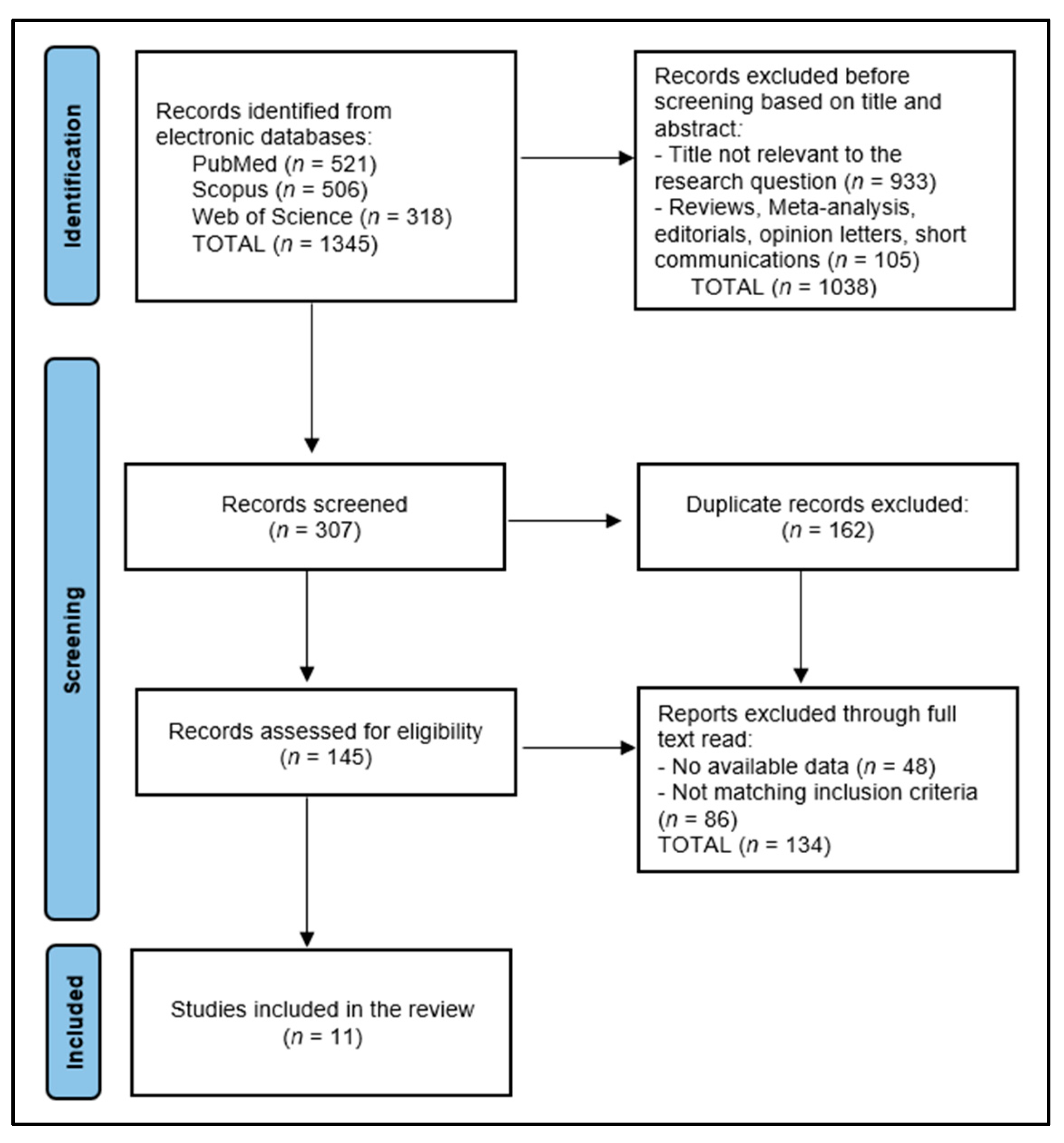
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Definitions
2.4. Data Collection Process
2.5. Risk of Bias and Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Patients’ Characteristics
3.3. Disease Characteristics
3.4. Outcomes and Quality of Life
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Przegląd Gastroenterol. 2019, 14, 89–103. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shin, A.E.; Giancotti, F.G.; Rustgi, A.K. Metastatic colorectal cancer: Mechanisms and emerging therapeutics. Trends Pharmacol. Sci. 2023, 44, 222–236. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chang, Y.Y.; Lin, P.C.; Lin, H.H.; Lin, J.K.; Chen, W.S.; Jiang, J.K.; Yang, S.H.; Liang, W.Y.; Chang, S.C. Mutation spectra of RAS gene family in colorectal cancer. Am. J. Surg. 2016, 212, 537–544.e3. [Google Scholar] [CrossRef]
- Saeed, O.; Lopez-Beltran, A.; Fisher, K.W.; Scarpelli, M.; Montironi, R.; Cimadamore, A.; Massari, F.; Santoni, M.; Cheng, L. RAS genes in colorectal carcinoma: Pathogenesis, testing guidelines and treatment implications. J. Clin. Pathol. 2019, 72, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, M.; Alabdullatif, N.; Al-Rashoud, A.; Alotaibi, J.; Alhussaini, N.; Elsirawani, S.; Somily, H.; Alkhudair, N.; AlOtaiby, M.; Ahamed, S.S.; et al. KRAS Mutations in Colorectal Cancer: Relationship With Clinicopathological Characteristics and Impact on Clinical Outcomes in Saudi Arabia. Cureus 2022, 14, e23656. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, F.; Lin, Y.; Li, R.; Shen, X.; ** Review. Patient Prefer. Adherence 2023, 17, 2679–2706. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fakih, M.G.; Salvatore, L.; Esaki, T.; Modest, D.P.; Lopez-Bravo, D.P.; Taieb, J.; Karamouzis, M.V.; Ruiz-Garcia, E.; Kim, T.W.; Kuboki, Y.; et al. Sotorasib plus Panitumumab in Refractory Colorectal Cancer with Mutated KRAS G12C. N. Engl. J. Med. 2023, 389, 2125–2139. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Zhao, M.; Tang, W.; Zheng, X. Impacts of systemic treatments on health-related quality of life for patients with metastatic colorectal cancer: A systematic review and network meta-analysis. BMC Cancer 2024, 24, 188. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Battaglin, F.; Puccini, A.; Ahcene Djaballah, S.; Lenz, H.J. The impact of panitumumab treatment on survival and quality of life in patients with RAS wild-type metastatic colorectal cancer. Cancer Manag. Res. 2019, 11, 5911–5924. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Peeters, M.; Price, T.J.; Cervantes, A. Randomized phase III studyof panitumumab with fluorouracil, leucovorin, and irinotecan(FOLFIRI) compared with FOLFIRI alone as second-line treatmentin patients with metastatic colorectal cancer. J. Clin. Oncol. 2010, 28, 4706–4713. [Google Scholar] [CrossRef] [PubMed]
- Hecht, J.R.; Cohn, A.; Dakhil, S.; Saleh, M.; Piperdi, B.; Cline-Burkhardt, M.; Tian, Y.; Go, W.Y. SPIRITT: A randomized, multicenter, phase II study of panitumumab with FOLFIRI andbevacizumab with FOLFIRI as second-line treatment in patientswith unresectable wild type KRAS metastatic colorectal cancer. Clin. Color. Cancer 2015, 14, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Peeters, M.; Oliner, K.S.; Price, T.J.; Cervantes, A.; Sobrero, A.F.; Ducreux, M.; Hotko, Y.; André, T.; Chan, E.; Lordick, F.; et al. Analysis of KRAS/NRASmutations in a phase III study of panitumumab with FOLFIRI compared with FOLFIRI alone as second-line treatment for metastaticcolorectal cancer. Clin. Cancer Res. 2015, 21, 5469–5479. [Google Scholar] [CrossRef] [PubMed]
- Therkildsen, C.; Bergmann, T.K.; Henrichsen-Schnack, T.; Ladelund, S.; Nilbert, M. The predictive value of KRAS, NRAS, BRAF, PIK3CA and PTEN for anti-EGFR treatment in metastatic colorectal cancer: A systematic review and meta-analysis. Acta Oncol. 2014, 53, 852–864. [Google Scholar] [CrossRef] [PubMed]
- Murakawa, Y.; Ootsuka, K.; Kusaka, J.; Miura, K. Correlation between overall survival and quality of life in colon cancer patients with chemotherapy. BMC Cancer 2023, 23, 492. [Google Scholar] [CrossRef]
- Chiang, T.Y.; Hsu, H.C.; Chern, Y.J.; Liao, C.K.; Hsu, Y.J.; Tsai, W.S.; Hsieh, P.S.; Lin, Y.F.; Lee, H.L.; You, J.F. Skin Toxicity as a Predictor of Survival in Metastatic Colorectal Cancer Patients Treated with Anti-EGFR: Fact or Fallacy? Cancers 2023, 15, 1663. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study & Author | Country | Study Year | Study Design | Study Quality |
|---|---|---|---|---|
| 1 Bennett et al. [31] | France | 2011 | Randomized trial | Medium |
| 2 Odom et al. [32] | United States | 2011 | Randomized trial | Medium |
| 3 Láng et al. [33] | Multinational | 2013 | Randomized trial | High |
| 4 Seymour et al. [34] | United Kingdom | 2013 | Randomized trial | High |
| 5 Yamaguchi et al. [35] | Multinational | 2017 | Randomized trial | Medium |
| 6 Shitara et al. [36] | Japan | 2019 | Randomized trial | High |
| 7 Pietrantonio et al. [37] | Italy | 2020 | Randomized trial | Medium |
| 8 Raimondi et al. [38] | Italy | 2020 | Randomized trial | Medium |
| 9 Ooki et al. [39] | Japan | 2022 | Randomized trial | High |
| 10 Bertaut et al. [40] | France | 2022 | Randomized trial | Medium |
| 11 Ballhausen et al. [41] | Germany | 2023 | Randomized trial | Medium |
| Study Number | Study Arm (s) | Control Arm (s) | Age, Years (Mean/Median) | Gender Distribution (Male) | Race (White) |
|---|---|---|---|---|---|
| 1 Bennett et al. [31] | Panitumumab + FOLFOX4 (n = 284) Panitumumab + FOLFIRI (n = 263) | FOLFOX4 alone (n = 292) FOLFIRI alone (n = 267) | 60.1–60.6 | 66.5% (Panitumumab + FOLFOX4) 63.7% (FOLFOX4 alone) 60.5% (Panitumumab + FOLFIRI) 64.0% (FOLFIRI alone) | 90.5–97.0% |
| 2 Odom et al. [32] | Panitumumab plus BSC (n = 188) | BSC alone (n = 175) | 61–62 | 65% | 98–99% |
| 3 Láng et al. [33] | FOLFIRI + Cetuximab (n = 300) | FOLFIRI (n = 327) | 60 | 62–63% | NR |
| 4 Seymour et al. [34] | IrPan (n = 230) | Irinotecan (n = 230) | 63–64 | 69–70% | NR |
| 5 Yamaguchi et al. [35] | Cetuximab + FOLFIRI (n = 170) | FOLFIRI alone (n = 181) | 59–60 | 63.5–65.7% | NR |
| 6 Shitara et al. [36] | Regorafenib followed by Cetuximab ± Irinotecan (R-C arm) (n = 51) | Cetuximab ± Irinotecan followed by Regorafenib (C-R arm) (n = 50) | 65–68 | 61–66% | NR |
| 7 Pietrantonio et al. [37] | Capecitabine plus temozolomide (CAPTEM) (n = 43) | FOLFIRI (n = 43) | 67–70 | CAPTEM: 42% FOLFIRI: 56% | 100% |
| 8 Raimondi et al. [38] | Panitumumab plus 5-FU/LV (Arm A) (n = 107) | Panitumumab (Arm B) (n = 10.3) | 63.5 | 65.7% | 100% |
| 9 Ooki et al. [39] | Cetuximab plus chemotherapy (n = 128) | NR | 66 | 68.0% | 100% |
| 10 Bertaut et al. [40] | Bevacizumab + chemotherapy (mFOLFOX6 or FOLFIRI) (n = 65) | Cetuximab + chemotherapy (mFOLFOX6 or FOLFIRI) (n = 67) | NR | NR | NR |
| 11 Ballhausen et al. [41] | Panitumumab (n = 53) | Fluorouracil + Folinic Acid (n = 48) | NR | NR | NR |
| Study Number | Disease Duration/Follow-Up | Performance Status | Primary Tumor | Metastasis Site (s) | RAS Mutation |
|---|---|---|---|---|---|
| 1 Bennett et al. [31] | Follow-up monthly until disease progression | ECOG 0–1: 94.5–96.2% | Colon: 60.8–65.8% Rectum: 35.6–39.2% | Liver only: 17–21% Liver + other: 63–68% Other only: 13–15% | Wild-type KRAS: 100% |
| 2 Odom et al. [32] | Time since primary diagnosis: 31–33 months (mean) Time since metastatic disease: 19–24 months (mean) | ECOG 0: 35–48% ECOG 1: 40–52% ECOG 2: 11–15% | Colon: 67% Rectum: 33% | NR | Wild-type: 60.6% Mutant: 39.4% |
| 3 Láng et al. [33] | Follow-up every 3 months until disease progression | ECOG 0: 57–59% ECOG 1: 37–39% ECOG 2: 4% | Colon: 67–70% Rectum: 30–33% | Liver metastases only: 21–23% | Wild-type KRAS: 100% |
| 4 Seymour et al. [34] | Median follow-up 25.4 months | WHO 0–1: 94% WHO 2: 6% | Right colon: 27–32% Left colon: 29–36% Rectum: 35–36% | Liver: 72–76% Lung: 50–54% | Wild-type KRAS: 100% |
| 5 Yamaguchi et al. [35] | Follow-up every 8 weeks, up to 32–40 weeks | ECOG 0: 55.9–60.2% ECOG 1: 35.9–41.2% ECOG 2: 2.9–3.9% | NR | Liver metastases: 23.8–24.7% More than two sites involved: 8.2–13.3% | Wild-type KRAS: 100% |
| 6 Shitara et al. [36] | Median follow-up 29 months. Assessment every 4 weeks. | ECOG PS 0: 67% in R-C, 78% in C-R ECOG PS 1: 33% in R-C, 22% in C-R | Left-side: 75% in R-C, 86% in C-R; Right-side: 25% in R-C, 14% in C-R | Liver: 63% in R-C, 62% in C-R; Lung: 59% in R-C, 46% in C-R; Lymph node: 41% in R-C, 48% in C-R; Peritoneum: 22% in R-C, 18% in C-R | Wild-type in circulating tumor DNA (ctDNA) at study entry: 90% in R-C arm, 88% in C-R arm; Mutant: 8% in both arms |
| 7 Pietrantonio et al. [37] | Median follow-up 30.5 months. QoL assessment every 8 weeks. | ECOG 0: 56% in CAPTEM, 51% in FOLFIRI; ECOG 1: 44% in CAPTEM, 49% in FOLFIRI | Right side: 35% in CAPTEM, 40% in FOLFIRI; Left side: 65% in CAPTEM, 60% in FOLFIRI | Synchronous metastases 72% (CAPTEM) vs. 67% (FOLFIRI) >1 metastatic sites 58% (CAPTEM) vs. 65% (FOLFIRI) | RAS-mutated, MGMT-methylated mCRC 100% |
| 8 Raimondi et al. [38] | Follow-up for 40 weeks. Assessments every 8 weeks. | ECOG 0: 73.8% ECOG 1: 26.2% | Left-sided (84.3%) vs. Right-sided (15.7%). | Liver-limited disease in 35.2% of patients, peritoneal metastasis in 22.9%. | Wild-type RAS: 100% |
| 9 Ooki et al. [39] | Assessments at 2, 4, 8, 16, and 24 weeks for QoL and every 8 weeks for radiologic assessments. | ECOG 0: 83.6% ECOG 1: 16.4% | Colon: 64.8% Rectum: 35.2% | ≥2 metastases 64.0% | Wild-type KRAS: 100% |
| 10 Bertaut et al. [40] | Assessment 1 and 3 (approximately 6 and 18 weeks after initial treatment) Median follow-up time 4.1 months for bevacizumab group vs. 1.7 months cetuximab group | WHO 0–1: 100% | NR | NR | Wild-type RAS: 100% |
| 11 Ballhausen et al. [41] | 10 treatment cycles | ECOG 0–1: 100% | NR | NR | Wild-type RAS: 100% |
| Study Number | Baseline Results | QoL Follow-Up Results | Complications/Drop-out/Survival | Conclusions |
|---|---|---|---|---|
| 1 Bennett et al. [31] | EQ-5D HSI Mean: 0.76–0.78 EQ-5D VAS Mean: 70.1–74.1 | Improvement in EQ-5D scores not clinically meaningful | Late dropout/completer: 48–52% (Panitumumab + FOLFOX4); 37.4–62.6% (FOLFOX4 alone); 39.7–60.3% (Panitumumab + FOLFIRI); 29.8–70.2% (FOLFIRI alone) | Addition of panitumumab to chemotherapy (FOLFOX4 or FOLFIRI) in wild-type KRAS mCRC did not compromise QoL significantly and improved significantly the DFS. |
| 2 Odom et al. [32] | FCSI Score Mean: 72.27–73.21 (Panitumumab + BSC) 71.84–71.91 (BSC alone) EQ-5D Index Mean: 0.68–0.73 | Improvement in FCSI and EQ-5D Index scores favored Panitumumab + BSC, especially in wild-type KRAS mCRC | Early dropout: 38–42% (Panitumumab + BSC), 68% (BSC alone) Late dropout/completer: 57–62% (Panitumumab + BSC), 31–32% (BSC alone) | Panitumumab-treated patients with wild-type KRAS mCRC maintained better control of CRC symptoms and quality of life compared with BSC alone. |
| 3 Láng et al. [33] | NR | Worsened nausea and vomiting at week 16 (FOLFIRI vs. FOLFIRI + Cetuximab: 14.25 vs. 9.08). A worse change from baseline score for dyspnea in the FOLFIRI + Cetuximab arm. Early skin reactions in patients receiving cetuximab did not significantly affect these QoL scales | Median survival 25.7 (cetuximab + FOLFIRI) vs. 16.4 months (FOLFIRI) (HR 1.68). Constant and similar compliance rates. Better tumor response 58% (cetuximab + FOLFIRI) vs. 40% FOLFIRI | Adding cetuximab to FOLFIRI did not significantly impact GHS/QoL or social functioning, despite improved response rates and survival. |
| 4 Seymour et al. [34] | NR | Grade 3 or worse diarrhea (29% vs. 18%), skin toxicity (19% vs. 0%), lethargy (21% vs. 11%), infection (19% vs. 10%), and hematological toxicity (22% vs. 12%) more common in IrPan group. | Progression-free survival longer in IrPan group (HR 0.78). Higher response rate in IrPan group (34% vs. 12%). Five treatment-related deaths reported (1.0%). | Adding panitumumab to irinotecan did not improve overall survival for patients with wild-type KRAS tumors, despite longer progression-free survival and higher response rate. |
| 5 Yamaguchi et al. [35] | Cetuximab + FOLFIRI vs. FOLFIRI GHS/QoL 60.9 vs. 61.9 Physical functioning 77.4 vs. 78.7 Fatigue 32.6 vs. 33.2 Nausea and vomiting 7.7 vs. 6.5 Pain 23.3 vs. 23.6 | Cetuximab + FOLFIRI vs. FOLFIRI GHS/QoL 65.0 vs. 68.6 Physical functioning 80.2 vs. 80.0 Fatigue 29.3 vs. 31.6 Nausea and vomiting 8.7 vs. 12.0 Pain 14.6 vs. 14.7 | High drop-out rate. | Adding cetuximab to FOLFIRI did not negatively impact QoL, while improving PFS, OS, and ORR in patients with RAS wild-type mCRC. Changes in GHS/QoL and social functioning from baseline to week 8 were similar irrespective of whether patients experienced early skin reactions. |
| 6 Shitara et al. [36] | NR | Average EQ-5D between the two arms after treatment (difference = −0.011). | Median OS significantly longer in R-C (17.4 months) vs. C-R (11.6 months), HR for OS was 0.61 (95% CI, 0.39–0.96). No unexpected safety signals were observed. | Regorafenib treatment resulted in worse mobility, pain/discomfort, self-care, and usual activity scores compared to cetuximab after 4 weeks in both treatment periods, particularly in the C-R arm. |
| 7 Pietrantonio et al. [37] | NR | QLQ-30 showed a significantly better QoL in CAPTEM arm +5.42 vs. −17.19 at 8 weeks, and +3.57 vs. −11.67 at 16 weeks. FACT-C showed a significantly better change from baseline in the CAPTEM arm +0.19 vs. −7.06 at 8 weeks, and −2.07 vs. −9.74 at 24 weeks. | Median PFS: 3.5 months for both arms; Median OS: 9.5 months for CAPTEM and 10.6 months for FOLFIRI; Grade 3 treatment-related adverse events higher in FOLFIRI (47.6%) vs. CAPTEM (16.3%) Mortality 65.1% in CAPTEM arm vs. 72.1% in FOLFIRI | CAPTEM regimen failed to show superiority over FOLFIRI. Better QoL in the CAPTEM arm. |
| 8 Raimondi et al. [38] | NR | Global QoL worsened in 40.9% in panitumumab plus5-FU/LV arm vs. 29.5% in panitumumab arm. | Compliance at baseline was high in both arms (Arm A: 91.5%, Arm B: 92.0%). Rates of patients completing questionnaires decreased over time. | Induction with oxaliplatin-containing chemotherapy plus anti-EGFRs leads to transient QoL deterioration, with overall recovery during maintenance, highlighting the impact of treatment deintensification on health-related QoL. |
| 9 Ooki et al. [39] | GHS/QoL 69 | ETS associated with improved QoL scores between baseline and 8 weeks: +5.86 for GHS/QoL, +26.73 for physical functioning, and +13.58 for social functioning in symptomatic patients. | Early tumor shrinkage achieved in 64.1% treated with cetuximab + chemotherapy. PFS was 10.8 months. 2-year OS 42.5% in symptomatic patients vs. 77.8% asymptomatic | ETS in patients treated with first-line cetuximab plus chemotherapy is associated with significant improvements in QoL for symptomatic patients, underscoring the importance of ETS in treatment efficacy and patient well-being. |
| 10 Bertaut et al. [40] | GHS/QoL 66.7 | GHS/QoL 62.5 Bevacizumab vs. 50.0 Cetuximab. | Median time to deterioration was 6 months. Diarrhea QLQ-C30 score is significantly higher in Bevacizumab. | No relevant impairment of patients QoL between the 2 treatment arms. |
| 11 Ballhausen et al. [41] | GHS/QoL 59.8 | GHS/QoL 59.8 | Appetite loss and diarrhea worsened in the Pman group. | The addition of Pmab to FU/FA as maintenance therapy prolongs DFS without negative impact on QoL. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Braicu, V.; Stelian, P.; Fulger, L.; Verdes, G.; Brebu, D.; Duta, C.; Fizedean, C.; Ignuta, F.; Danila, A.I.; Cozma, G.V. Impact of Systemic Treatments on Outcomes and Quality of Life in Patients with RAS-Positive Stage IV Colorectal Cancer: A Systematic Review. Diseases 2024, 12, 79. https://doi.org/10.3390/diseases12040079
Braicu V, Stelian P, Fulger L, Verdes G, Brebu D, Duta C, Fizedean C, Ignuta F, Danila AI, Cozma GV. Impact of Systemic Treatments on Outcomes and Quality of Life in Patients with RAS-Positive Stage IV Colorectal Cancer: A Systematic Review. Diseases. 2024; 12(4):79. https://doi.org/10.3390/diseases12040079
Chicago/Turabian StyleBraicu, Vlad, Pantea Stelian, Lazar Fulger, Gabriel Verdes, Dan Brebu, Ciprian Duta, Camelia Fizedean, Flavia Ignuta, Alexandra Ioana Danila, and Gabriel Veniamin Cozma. 2024. "Impact of Systemic Treatments on Outcomes and Quality of Life in Patients with RAS-Positive Stage IV Colorectal Cancer: A Systematic Review" Diseases 12, no. 4: 79. https://doi.org/10.3390/diseases12040079